Quick Primer Overview
How rare is pigmentary glaucoma?
Pigmentary glaucoma accounts for roughly 1% of all open-angle glaucoma cases. It tends to show up in young to middle-aged men, usually between their 20s and 40s. Even though its uncommon, the condition can progress quickly if left unchecked.
What causes pigmentary glaucoma?
The root of the problem is pigment dispersion syndrome (PDS). In PDS, tiny pigment granules slough off the back of the iris and drift into the eyes drainage system. When that pigment clogs the trabecular meshwork, intraocular pressure (IOP) can rise, leading to pigmentary glaucoma. In some cases, associated eye surface conditions like dry eye disease can worsen symptoms and make follow-up more important.
Pigmentary glaucoma symptoms
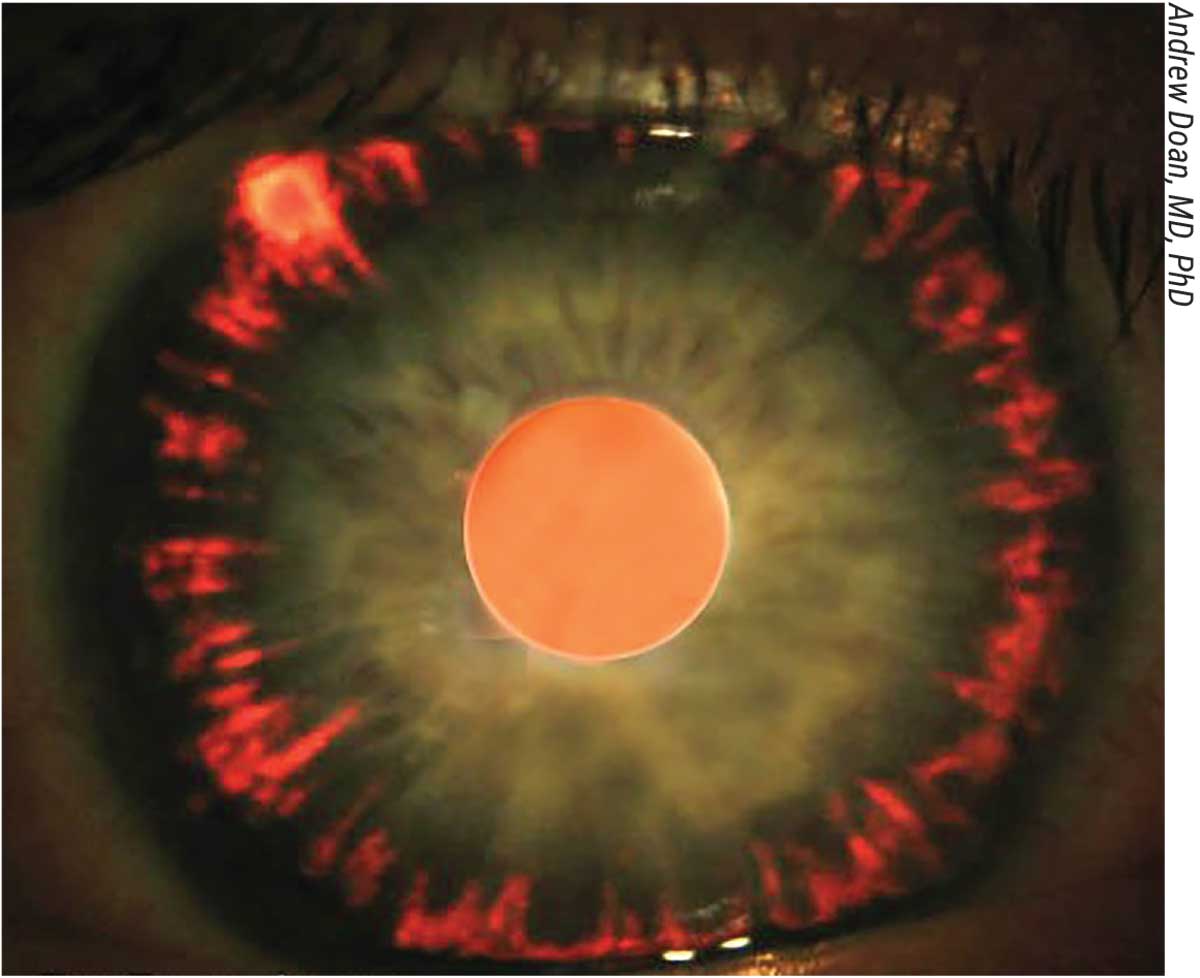
Early signs are often subtle: occasional blurry vision, halos around lights, or a mild ache behind the eye. Some people notice a Krukenberg spindlea vertical streak of pigment on the corneawhen their eye doctor dilates the pupils. If youve experienced any of these, its worth getting a thorough exam.
Pigment dispersion syndrome signs
Besides the Krukenberg spindle, clinicians look for mid-peripheral iris transillumination defects (tiny spots that let light through the iris) and a pigmented line on the corneal endothelium. Spotting these clues early can help catch pigmentary glaucoma before it damages the optic nerve.
Medication Therapy Guide
Which eye drops are preferred?
The first line of defense is usually prostaglandin analogues such as latanoprost or travoprost. These drops boost fluid outflow and can lower IOP by 2030%. If pressure remains high, doctors often add a beta-blocker (e.g., timolol) or a carbonic anhydrase inhibitor (e.g., dorzolamide) to the regimen.
How effective are drops for pigmentary glaucoma?
In most patients, a single prostaglandin can bring IOP down into the target range (<21mmHg). A real-world case I heard about involved a 28-year-old who stayed stable on latanoprost for two years, only needing a mild add-on once his pressure crept up.
Side-effects to watch for
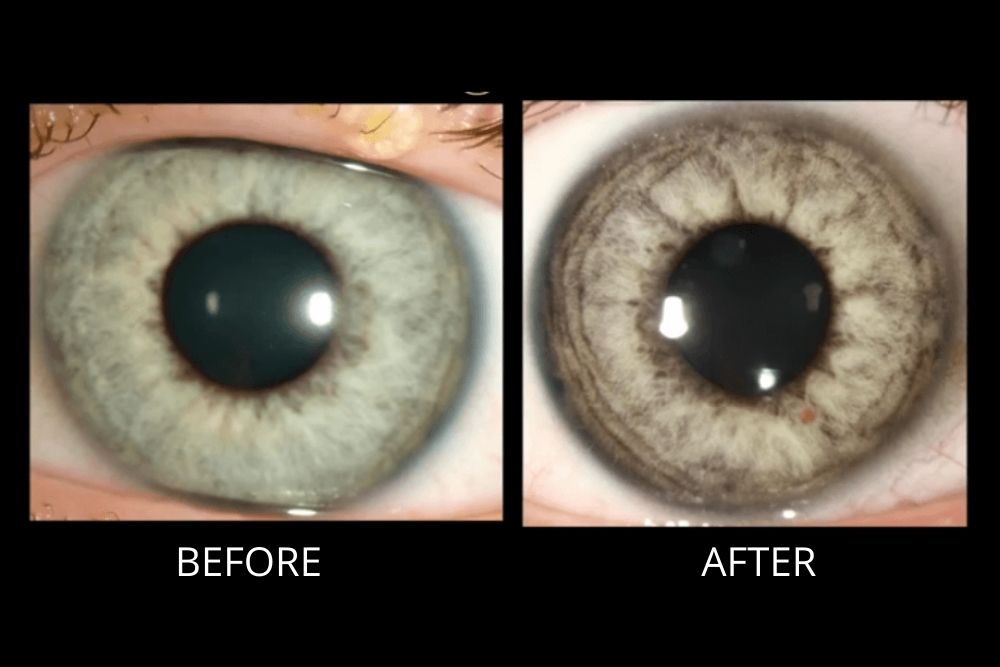
Prostaglandins can cause redness, increased eyelash growth, or a darkening of the irisusually harmless cosmetic changes. Beta-blockers may affect heart rate or lung function, so its vital to discuss any existing conditions with your ophthalmologist.
Laser Treatment Options
Selective Laser Trabeculoplasty (SLT) vs. Argon Laser Trabeculoplasty (ALT)
Both SLT and ALT target the drainage meshwork, helping it clear pigment and improve outflow. The cool thing about SLT is that it uses low-energy pulses, so the pigment actually assists the lasers jobmaking it especially useful for pigmentary glaucoma.
Studies report around a 70% success rate in maintaining target IOP after a single SLT session.
Laser Peripheral Iridotomy (LPI) for pigment dispersion
LPI creates a tiny hole in the peripheral iris, letting excess pigment flow out of the anterior chamber. Its most helpful when the iris is concave and the pigment is constantly shedding. The procedure is quickusually done in the officeand recovery is painless.
Risks & contraindications
Laser treatments can cause a temporary spike in IOP, mild inflammation, or, very rarely, a small bleed (hyphema). Your doctor will usually prescribe anti-inflammatory drops for a few days after the laser to keep things calm.
Surgical Intervention Choices
Trabeculectomy & tube shunt surgery
When medication and laser arent enough, surgeons may turn to trabeculectomy (creating a new drainage pathway) or implant a tube shunt. These are the gold standard for stubborn cases, but they come with a higher risk profilepotential infection, scarring, or the need for a revision surgery down the line.
Minimally Invasive Glaucoma Surgery (MIGS)
In recent years, MIGS devices like the iStent, Hydrus Microstent, and Trabectome have gained traction. Theyre smaller, cause less tissue disruption, and usually allow a quicker recovery. For pigmentary glaucoma, MIGS can lower pressure by about 1520% while keeping complications low.
| Procedure | Typical IOP Reduction | Complication Rate | Recovery Time |
|---|---|---|---|
| Trabeculectomy | 3040% | 1015% | 46 weeks |
| Tube Shunt | 2535% | 12% | 57 weeks |
| MIGS (iStent, Hydrus) | 1520% | 35% | 12 weeks |
Combination approaches
Many specialists start with drops, then add SLT or LPI, and only move to MIGS or trabeculectomy if pressure stays stubborn. This stepwise strategy is championed by major ophthalmology guidelines, which emphasize preserving vision while minimizing surgical risk.
Tailoring Treatment Plan
Factors influencing treatment choice
Your age, how advanced the glaucoma is, corneal health, how well you can stick to a drop schedule, and even insurance coverage all play a role. Younger patients often prefer laser or MIGS to avoid lifelong dependence on drops.
Sample treatment algorithm
Start Eye Drops Laser (SLT/LPI) MIGS Trabeculectomy/Tube. Your doctor will move you along this pathway based on how your IOP responds at each step.
Patient-centred conversation tips
Never hesitate to ask your eye doctor questions like, What are the chances this treatment will keep my pressure under control for the next five years? or If I choose surgery, what will my recovery look like? A transparent dialogue builds trust and helps you feel in control.
Prognosis and Management
Expected visual outcomes with optimal treatment
When the right regimen is followed, studies show that about 85% of patients maintain 20/40 vision or better over five years. The key is regular monitoringusually every 36 monthsto catch any pressure creep early.
Frequency of follow-up
After initial stabilization, most doctors recommend eye pressure checks and visual field testing at least twice a year. If youre on drops, youll likely need a slightly tighter schedule until your IOP is consistently low.
Lifestyle & self-care
Simple habits can support your treatment: stay hydrated, limit high-caffeine drinks (they can raise IOP), get regular moderate exercise, and avoid smoking. These tweaks wont replace medication, but they create a healthier environment for your eyes.
Bottom Line & Next Steps
In a nutshell, the best treatment for pigmentary glaucoma is usually a tiered approachstart with eye drops, move to laser if needed, and reserve surgery for the stubborn cases. Because every eye is unique, your doctor will craft a plan that balances effectiveness with safety, keeping your vision protected for years to come.
If you suspect pigmentary glaucoma, schedule a comprehensive eye exam today. Bring your questions, share any family history, and work together with your specialist to decide which of these options fits your lifestyle and eye health. Your eyes deserve the best carelet's make sure they get it.
FAQs
What are the first‑line medications for pigmentary glaucoma?
The initial therapy usually involves prostaglandin analogues (e.g., latanoprost or travoprost) which increase fluid outflow and lower intra‑ocular pressure.
When is laser therapy recommended over eye drops?
Laser treatments such as selective laser trabeculoplasty (SLT) are considered when target pressure isn’t reached with drops alone or when patients have difficulty maintaining a drop regimen.
Can a laser peripheral iridotomy (LPI) stop pigment dispersion?
LPI creates a small opening in the peripheral iris, allowing excess pigment to exit the anterior chamber. It’s most helpful for eyes with a concave iris that continually shed pigment.
What are the benefits of minimally invasive glaucoma surgery (MIGS) for pigmentary glaucoma?
MIGS devices like the iStent or Hydrus Microstent lower pressure by about 15‑20 % with a lower complication rate and faster recovery compared with traditional trabeculectomy.
How often should I have follow‑up appointments after starting treatment?
After the pressure is stabilized, most ophthalmologists schedule visits every 3‑6 months to monitor IOP, visual fields, and optic nerve health.