If your teen has suddenly started limping or complains of a deep hip ache, the dreaded phrase slipped capital femoral epiphysis (SCFE) might be lurking behind those symptoms. The fastest way to stop the slip and protect a growing hip is usually a brief, minimallyinvasive surgery. Below youll find the straighttothepoint facts about why that surgery is often needed, what the alternatives are, and how to weigh the benefits and risks for a safe, lasting recovery.
Why Treatment Matters
What Happens If SCFE Is Left Untreated?
Leaving a slipped capital femoral epiphysis unchecked is like ignoring a crack in a dam the damage spreads. Untreated slips can lead to:
- Avacular necrosis (the death of bone tissue)
- Earlyonset arthritis, making the hip painful even for simple chores
- Limblength discrepancy, so one leg ends up longer than the other
- Reduced range of motion that may never fully recover
What Are the Primary Goals of Treatment?
In a nutshell, the treatment aims to:
- Stabilize the epiphysis (the ball of the hip joint) so it stops sliding
- Prevent further damage to the blood supply
- Preserve as much natural hip function as possible for years to come
Standard Surgical Fixation
What Does a Limited Open Surgery Involve?
Think of it as a miniopen procedure. The surgeon makes a small incisionabout the size of a thumband inserts a single metal screw or pin across the growth plate to lock the femoral head in place. The technique is called insitu fixation and has become the gold standard because its quick, effective, and spares most of the surrounding tissue.
How Long Does SCFE Surgery Take?
On average the operation itself lasts 4590 minutes. Add about 30 minutes for anesthesia induction and a short recovery period in the postanesthesia care unit, and most families can head home the same day. A study published in the confirms that sameday discharge is safe for the majority of stable SCFE cases.
Typical Recovery Timeline
Recovery is a marathon, not a sprint, but the checkpoints are predictable:
- 02 weeks: Weightbearing is limited (usually crutches only). Pain is managed with prescribed medication and ice.
- 26 weeks: Gradual increase in weightbearing as the surgeon confirms the screw is holding firm on Xray.
- 36 months: Full return to sports and vigorous activities if the hip has healed properly and strength is back.
Alternative & Adjunct Treatments
Can SCFE Be Treated Without Surgery?
The short answer: rarely, and only in very early, stable slips. Nonoperative tricks like gentle traction or strict activity restriction may buy a few weeks, but they dont address the underlying instability. In practice, SCFE treatment without surgery is more of a theoretical footnote than a reliable pathway.
Role of Physiotherapy & WatchandWait Strategies
Physiotherapy can certainly help with pain and mobility, but its an adjunct, not a replacement. A watchandwait approach is sometimes used when the slip is minuscule and the child can bear weight without severe pain. Even then, the surgeon will keep a close eye on radiographs every 23 weeks to ensure the slip isnt worsening.
Specialized Surgical Options for Complex Cases
When Is a Realignment (Osteotomy) Needed?
If the slip is moderate to severe, the femoral head may sit at an awkward angle that a single screw cant correct. In those cases, surgeons may perform an osteotomycutting and reshaping the femurto realign the joint. This is a more involved operation, often requiring a longer hospital stay and a cautious rehab plan.
Imhauser Osteotomy & Surgical Hip Dislocation
The Imhauser technique is a threeplane osteotomy that corrects the angle of the femoral neck, while a surgical hip dislocation lets the surgeon see the joint from the inside. Both are powerful tools, but they come with higher risks such as blood loss, longer recovery, and a small chance of avascular necrosis. Thats why theyre reserved for patients where insitu fixation alone wont give a functional hip.
Contralateral (Prophylactic) Pinning Who Should Consider It?
Kids with risk factorsobesity, endocrine disorders (like hypothyroidism), or a family history of SCFEsometimes develop a slip in the other hip months or years later. Some surgeons recommend a preventive screw in the healthy side, especially if the child is still growing rapidly. The decision is always a shared one, weighing the tiny surgical risk against the potential of a future emergency.
PreOp Evaluation What Parents Should Ask Their Surgeon
Key Diagnostic Tests
Understanding the exact position of the slip is crucial. The usual workup includes:
- Plain Xray (AP and frogleg lateral views) the backbone of diagnosis.
- MRI helps spot early slips before theyre obvious on Xray and assesses blood flow to the femoral head.
- CT scan rarely needed, but useful for complex threedimensional planning.
Stable vs. Unstable SCFE What Does It Mean for You?
A stable slip means the child can bear weight (even with a limp). An unstable slip is when the child cant put any weight on the leg without severe pain. Unstable SCFE carries a higher risk of avascular necrosis and often requires urgent surgical fixation, sometimes combined with a gentle traction before the operation.
Questions to Ask the Orthopedic Team
Dont be shyyour surgeon wants you informed. Good questions include:
- How many SCFE surgeries have you performed in the past year?
- What is your success rate for insitu fixation?
- What are the common complications I should watch for after surgery?
- Will my child need a second operation to remove the screw later?
- What does the postop rehab plan look like, and how can we support it at home?
PostSurgical Care Maximizing Safety & Outcomes
Immediate PostOp Care
Right after the procedure, focus on pain control (often a combination of acetaminophen and a short course of opioids) and wound care. Keep an eye out for redstreaking, swelling, or a sudden increase in painthese could be signs of infection or hardware failure.
Rehabilitation Phases
Rehab is split into three clear stages:
| Phase | Time Frame | Goals & Activities |
|---|---|---|
| Phase1 | 06weeks | Protected weightbearing, gentle rangeofmotion (ROM) exercises, pain management. |
| Phase2 | 612weeks | Progressive strengthening (quadriceps, glutes), gait training, lowimpact cardio (stationary bike). |
| Phase3 | 36months | Sportspecific drills, agility work, clearance for full activity based on functional testing. |
LongTerm Monitoring
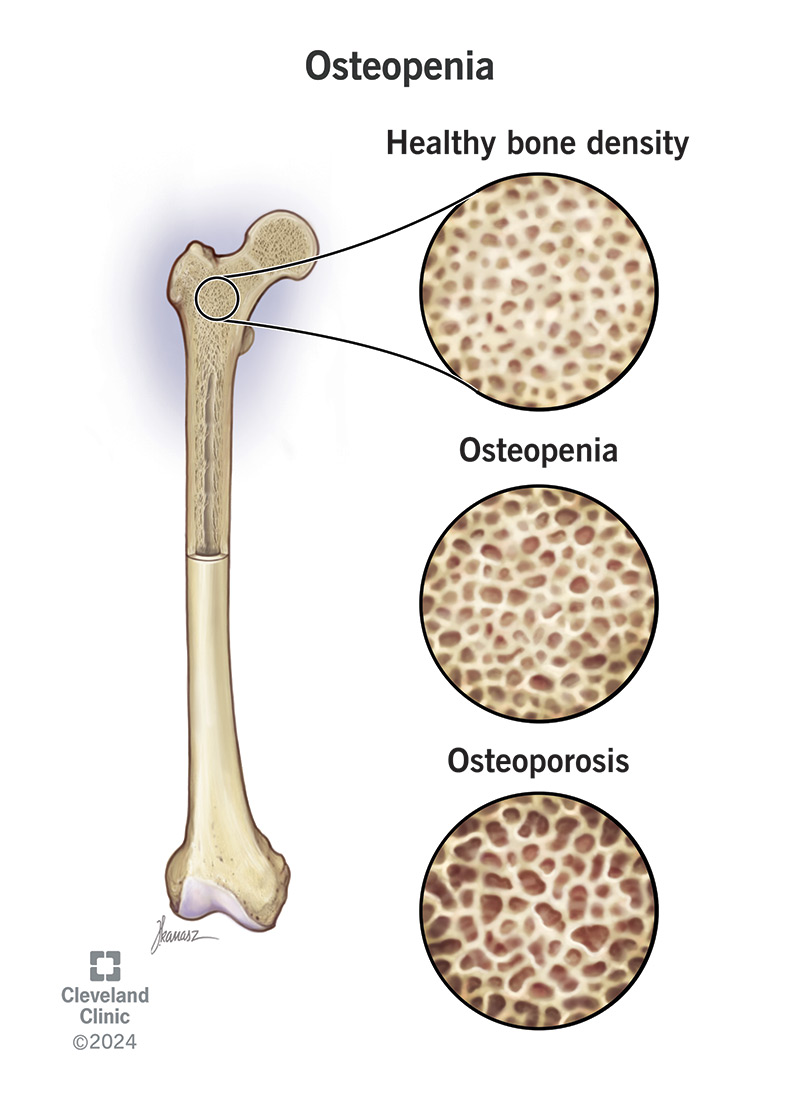
Even after the hip feels back to normal, the story isnt over. Annual Xrays are recommended until the growth plates close, to ensure the screw remains secure and the opposite hip stays healthy. If a contralateral slip is spotted early, treatment can be started before pain strikes. Parents who are concerned about bone health during recovery may also find guidance on osteoporosis bone density useful when discussing long-term bone-strengthening strategies with their clinician.
Frequently Asked Questions (Quick Answers)
How Old Is a Child Typically When SCFE Occurs?
Most cases appear between ages 11 and 14 in boys and a year or two later in girls, coinciding with the rapid growth spurt of puberty.
What Are the Most Common Symptoms?
A sudden limp, vague groin or thigh pain, and sometimes a stiff feeling when trying to swing the leg forward. The pain often worsens with activity and eases with rest, but it can be constant in unstable slips.
Is There Any NonSurgical Way to Prevent a Slip in the Future?
Weight management and regular screening for endocrine disorders are the most practical preventative steps. If a child is obese, even a modest reduction in body mass can lower the mechanical stress on the growth plate.
What Are the Success Rates of InSitu Screw Fixation?
Recent multicenter datacollated by the American Academy of Orthopaedic Surgeonsshow a success rate of over 90% in preventing further slippage and preserving hip function when performed within a few weeks of diagnosis.
Can the Hardware Be Removed Later, and Does That Affect Recovery?
Yes, many surgeons recommend removing the screw once the growth plate has closed (usually a few years after fixation). Removal is a minor outpatient procedure and does not typically compromise the healed hip.
RealWorld Perspectives Experience & Case Studies
Short Patient Story
Eightyearold Maya, an avid gymnast, started limping after a practice session. Xray revealed a mild SCFE. She underwent insitu fixation, spent two weeks in a protective boot, and followed a structured physiotherapy plan. One year later shes back on the balance beam, painfree, and her parents praise the clear communication they received from their surgeon.
Surgeon Insight
Dr. Patel, a pediatric orthopedic specialist at a major university hospital, explains why limited open surgery remains the goto technique: Its quick, the incision is tiny, and the screw gives the growth plate immediate stability. For most stable slips, thats all the child needs to get back to a normal life. He adds that meticulous preop imaging and honest discussions about risks are essential for building trust.
Data Snapshot
A recent review of 1,200 SCFE cases reported a 2% overall complication rate for insitu fixation, compared with 7% for more extensive osteotomies. The same study highlighted that obesity was the single largest predictor of a contralateral slip, underscoring the importance of lifestyle counseling.
Resources & Trusted References
Professional Guidelines
For the most uptodate clinical recommendations, consult the and the orthopedic departments. Both organizations provide patientfriendly fact sheets and videos that break down the anatomy and treatment steps.
PatientFocused Portals
Websites such as Childrens Hospital of Philadelphia and Seattle Childrens Hospital host detailed SCFE overviews, including agespecific symptom checklists and postop rehabilitation videos.
Academic Articles for Deeper Dive
For clinicians and curious parents, the peerreviewed article Current Management Strategies for Slipped Capital Femoral Epiphysis offers a comprehensive review of surgical techniques, longterm outcomes, and emerging research.
Conclusion
Discovering that your child has slipped capital femoral epiphysis can feel like a sudden, scary drop into the deep end of medical jargon. The good news is that, in most cases, a short, minimallyinvasive surgerycombined with a thoughtful rehab planlocks the hip in place and sets the stage for a healthy, active future. While nonsurgical options exist, theyre rarely definitive, and the risk of longterm complications (like early arthritis) usually outweighs any shortterm comfort.
Our top recommendation? If you notice any unexplained limp, groin pain, or sudden difficulty walking in a growing child, seek an orthopedic evaluation right away. Early diagnosis, clear communication with a trusted surgeon, and a balanced approach to treatment will give your teen the best chance at a painfree, active life.
FAQs
What is the standard surgical treatment for slipped capital femoral epiphysis?
The most common surgery is in situ fixation, a minimally invasive procedure where a single screw or pin is inserted to stabilize the slipped femoral epiphysis and prevent further slipping.
Can slipped capital femoral epiphysis be treated without surgery?
Non-surgical treatment is rarely effective and usually only considered for very early, stable slips. Most cases require surgery to stabilize the hip and prevent serious complications.
What is the typical recovery timeline after SCFE surgery?
Weight-bearing is usually limited for the first 2 weeks, gradually increasing over 2 to 6 weeks, with full return to sports and vigorous activity often taking up to 3 to 6 months or longer depending on healing.
When is an osteotomy recommended in SCFE treatment?
Osteotomy, a surgical realignment procedure, is reserved for moderate to severe slips where the femoral head angle is abnormal and cannot be adequately corrected by simple pinning.
Should the opposite hip be treated preventively in SCFE?
Prophylactic pinning of the contralateral hip may be recommended for children with risk factors like obesity or endocrine disorders to prevent a future slip, but the decision is individualized and discussed with the surgeon.