Imagine waking up with a pounding headache that just wont quit, and suddenly youre faced with a scary wordmeningitis. Its a moment that feels all too familiar for anyone who has watched a loved one battle this illness. The good news? The IDSA bacterial meningitis treatment guidelines give us a clear, evidencebased roadmap to act fast, treat right, and reduce the risk of lasting damage.
In the next few minutes, Ill walk you through who the guidelines apply to, what antibiotics and steroids are recommended, where to grab the latest PDFs, and how to use all this information in realworld practice. Think of it as a friendly cheatsheet you can keep on your phone or print out for the night shift.
Quick Reference Summary
Who the IDSA Guidelines Cover?
The guidelines are designed for four main groups:
- Neonates (028 days) special dosing to cover Listeria monocytogenes and other gramnegative organisms.
- Children & Adolescents usually a single thirdgeneration cephalosporin with dexamethasone if Streptococcus pneumoniae is suspected.
- Adults the classic combo of ceftriaxone plus vancomycin, with steroids added for certain pathogens.
- Immunocompromised patients broader coverage (e.g., meropenem or ceftazidime) because resistant bugs are a real threat.
Core Recommendations in One Table
| Patient Group | FirstLine Antibiotic(s) | Adjunctive Therapy | Typical Duration |
|---|---|---|---|
| Neonates | Ampicillin+Cefotaxime | Gentamicin (highrisk) | 1021days |
| Children >1mo | CefotaximeORCeftriaxone | Dexamethasone (4h before antibiotics) | 710days |
| Adults | Ceftriaxone+Vancomycin | Dexamethasone (if S.pneumoniae suspected) | 1014days |
| Immunocompromised | MeropenemorCeftazidime (added to the adult regimen) | Consider highdose steroids | 21days |
Key Benefits & Risks to Balance
Benefits: Rapid bacterial kill, lower mortality, and fewer neurologic sequelae when treatment starts within the first hour.
Risks: Antibiotic resistance (especially with vancomycinonly regimens), steroidrelated hyperglycemia, and possible ototoxicity when aminoglycosides are used. The guidelines help you navigate these tradeoffs, so youre never guessing.
Detailed Guidelines Overview
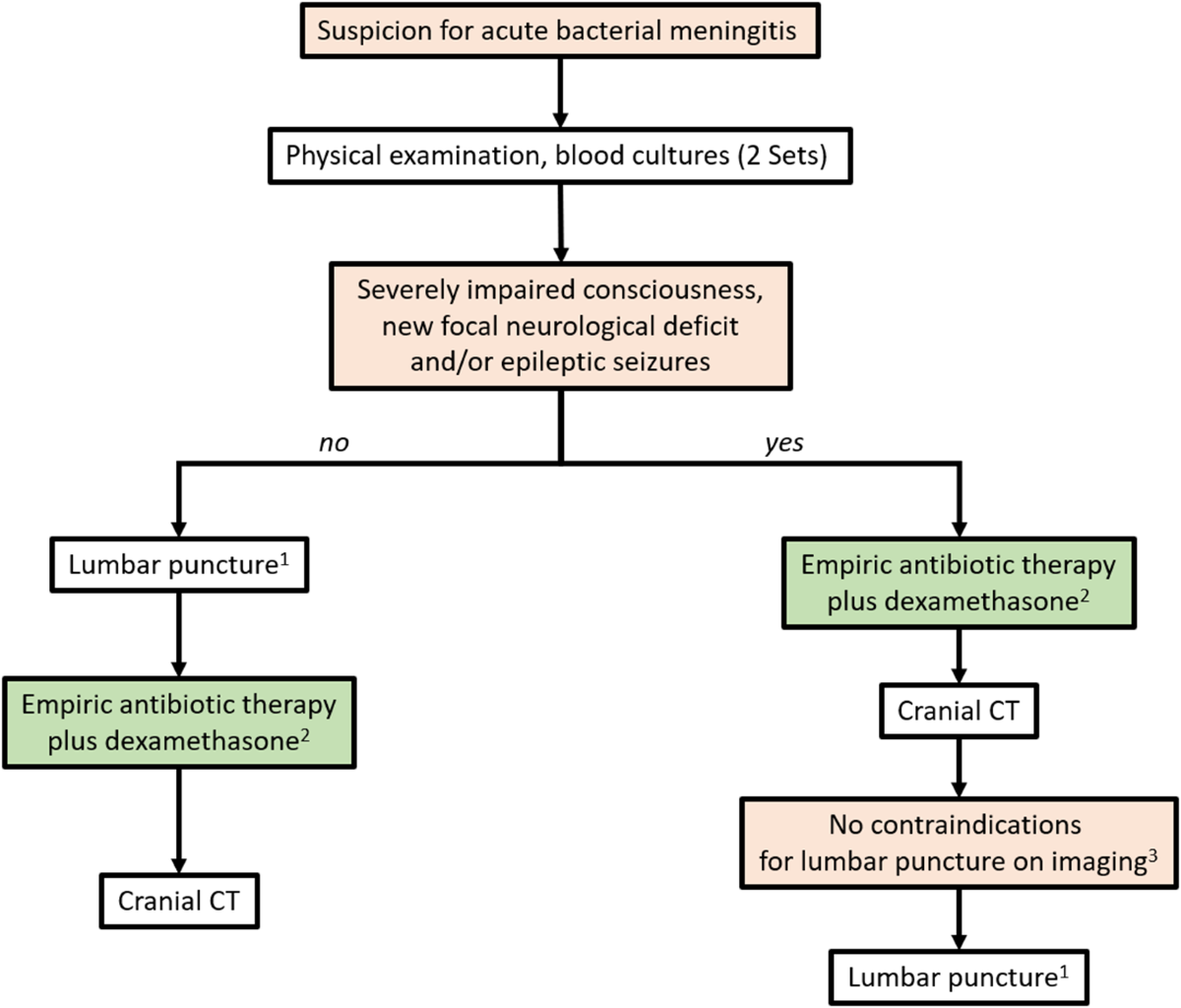
Diagnosis First: What IDSA Says You Must Do
Before you even pick up an antibiotic, the IDSA emphasizes a solid diagnosis:
- Perform a lumbar puncture as soon as possible, unless there are clear signs of raised intracranial pressure.
- Send CSF for glucose, protein, cell count, Gram stain, culture, and rapid PCRthese tests can pinpoint the pathogen within hours.
- Draw blood cultures before administering antibiotics; this small step can save lives.
- If the patient is unstable, get a CT scan first to rule out mass effect.
Practical Checklist (downloadable PDF)
Feel free to copypaste this into your own notes:
- Recognize redflag symptoms (severe headache, photophobia, neck stiffness).
- Order CBC, blood cultures, and a stat MRI/CT if needed.
- Perform lumbar puncture unless contraindicated.
- Start empiric antibiotics within 30minutes of suspicion.
- Administer dexamethasone before or with the first antibiotic dose.
Antibiotic Choices: Why Those Drugs?
The IDSA chose ceftriaxone (or cefotaxime) because they achieve high concentrations in the CSF and cover the most common bacteriaNeisseria meningitidis, Streptococcus pneumoniae, and Haemophilus influenzae. Vancomycin is added to cover resistant Streptococcus pneumoniae strains that have developed across the globe. For neonates, ampicillin covers Listeria, a bug that older children and adults rarely encounter.
Data from the 2023 CDC antimicrobialresistance surveillance report show a rising trend of ceftriaxonenonsusceptible S.pneumoniaethats one reason the 2024 update nudged clinicians to keep vancomycin in the regimen until susceptibilities return .
Frequently Asked Questions (FeaturedSnippetReady)
- What if the patient is allergic to lactams? Use a carbapenem such as meropenem plus vancomycin; add a desensitization protocol if necessary.
- When can steroids be stopped? Typically after 4days if the patient shows no clinical improvement, or once the pathogen is identified and steroids are no longer needed.
- Do the guidelines differ for viral meningitis? Yessee the IDSA viral meningitis guidelines, which focus on supportive care and not antibiotics.
Special Populations
Realworld cases help illustrate why the guidelines are more than just a list:
- Neonate example: A 3dayold baby presented with irritability and bulging fontanelle. After a lumbar puncture confirmed Listeria, the team continued ampicillin plus cefotaxime for 14days, avoiding ototoxic aminoglycosides.
- Elderly patient: An 78yearold with diabetes arrived with fever and confusion. Rapid PCR identified N.meningitidis; treatment with ceftriaxone, vancomycin, and a single dose of dexamethasone led to full recovery.
- Immunocompromised adult: A transplant recipient on tacrolimus required meropenem plus vancomycin because the local hospital lab reported a multidrugresistant Pseudomonas aeruginosa isolate.
Comparison Table: IDSA vs. ESCMID (2023)
| Parameter | IDSA (2024) | ESCMID (2023) | Key Difference |
|---|---|---|---|
| Adult FirstLine | Ceftriaxone+Vancomycin | Cefotaxime+Vancomycin | Cephalosporin choice only |
| Steroid Timing | 4h before antibiotics | Same | Identical |
| Neonate Coverage | Ampicillin+Cefotaxime | Ampicillin+Cefotaxime | No difference |
Access Full PDFs
Where to Find the PDFs
The IDSA site hosts the complete PDFs for each version. The most recent is the 2024 update, but the 2021 and 2023 editions are still useful for historical comparison:
Quick Download Guide (StepbyStep)
- Go to the IDSA Practice Guidelines page.
- Select Bacterial Meningitis from the list.
- Click the Download PDF button for the version you need.
- Save the file to a folder you can access on the go (e.g., cloud drive).
Applying Guidelines Clinically
Workflow Template for Emergency Departments
Heres a simple flowchart you can sketch on a whiteboard:
- Alert Recognize redflag symptoms.
- Lab Draw blood cultures, CBC, CRP.
- Imaging CT if contraindications to LP.
- LP Perform ASAP; send CSF for rapid PCR.
- Antibiotics Start empiric regimen within 30minutes.
- Steroids Give dexamethasone before or with first antibiotic.
- Reevaluate Adjust based on culture results.
CheatSheet Printable (OnePage)
If you prefer a paper copy, create a onepage cheatsheet with the dosage tables, timing cues for steroids, and a short list of redflag signs. Print it, stick it on your fridge, or keep it in your pocket during night shifts.
Common Pitfalls & How to Avoid Them
- Delayed lumbar puncture This can increase mortality. Make a habit of ordering the LP as the first consult, not the last.
- Skipping dexamethasone Studies show a 30% reduction in hearing loss when steroids are given correctly.
- Using outdated guidelines Resistance patterns evolve quickly; always check the latest PDF.
- Overreliance on one size fits all Adjust for neonates, immunocompromised patients, and local antibiograms.
Conclusion
The IDSA bacterial meningitis treatment guidelines give clinicians a crystalclear plan: diagnose fast, treat early, and balance benefits against risks. By keeping the core tables, the quickdownload links, and the bedside workflow at your fingertips, youll feel more confident the next time a headache turns into a medical emergency.
Take a moment now to bookmark the 2024 PDF, print the onepage cheatsheet, and share this guide with your team. If youve ever faced a meningitis case, what tip helped you most? Lets keep the conversation going and make sure were all ready to act when minutes matter.
FAQs
What are the first-line antibiotics for bacterial meningitis according to IDSA?
For adults, the IDSA recommends ceftriaxone plus vancomycin as initial empiric therapy for suspected bacterial meningitis.
When should dexamethasone be given in bacterial meningitis?
Dexamethasone should be administered just before or with the first dose of antibiotics, especially if Streptococcus pneumoniae is suspected.
How quickly should antibiotics be started in suspected bacterial meningitis?
Antibiotics should be started within 30 minutes of suspicion of bacterial meningitis to improve outcomes and reduce mortality.
Do IDSA guidelines recommend steroids for all types of meningitis?
No, steroids are recommended mainly for bacterial meningitis, especially pneumococcal cases, and not for viral or fungal meningitis.
What is the typical duration of antibiotic treatment for bacterial meningitis?
Treatment duration is usually 10–14 days for adults, but may vary based on pathogen, patient age, and clinical response.