Imagine youve just taken a deep breath after a night of wheezing, only to hear your doctor say the airways have changed permanently. Thats asthma structural remodeling, and its the reason some people stop responding to inhalers.
In short, airway remodeling is the hardwired thickening and scarring of the airway wall that can limit lung function, but we now know why it happens, how to spot it early, and what can be done to slow or even reverse it. For people with cystic fibrosis, understanding cystic fibrosis airway clearance techniques is equally important, as clearing mucus plays a critical role in maintaining airway health.
What It Is
Definition and Key Components
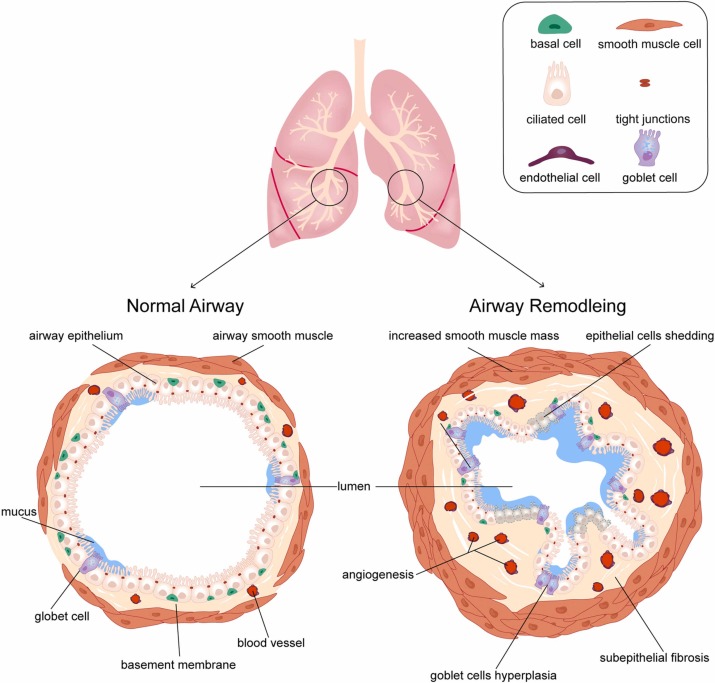
Asthma structural remodeling refers to a collection of permanent changes in the bronchial wall. Think of the airway like a flexible straw; over time, the straws walls become thicker, less elastic, and sometimes even develop extra ridges. The main players are:
- Subepithelial fibrosis collagen builds up just beneath the lining.
- Smoothmuscle hypertrophy the muscle layer gets bulkier.
- Gland enlargement mucusproducing glands grow larger.
- Neovascularisation new tiny blood vessels sprout.
- Epithelial injury the surface gets damaged and slower to heal.
How It Differs From Airway Inflammation
Inflammation is the bodys shortterm alarm systemred, hot, and reversible with steroids. Remodeling is the longterm construction work that stays even after the alarm settles.
| Feature | Inflammation | Remodeling |
|---|---|---|
| Reversibility | Usually reversible | Often permanent |
| Primary Cause | Allergens, irritants | Chronic inflammation, genetics |
| Diagnostic Marker | Elevated eosinophils, FeNO | Wall thickening on CT |
Why It Happens
Chronic Inflammation Pathways
When asthma is left unchecked, immune cells keep releasing cytokines like IL4, IL13, IL17, and the master fibrostimulator TGF. These messengers tell airway cells to lay down more collagen and muscleessentially turning a soft sponge into a rigid tube.
Environmental and Lifestyle Triggers
Allergens, viral infections, tobacco smoke, and even occupational chemicals act like nonstop construction crews, accelerating the remodeling process. If youve ever noticed that a cold seemed to linger longer in your asthmatic lungs, thats a clue.
Genetic and Epigenetic Predisposition
Recent genomewide association studies have identified several genes that make some people more prone to thickened airways. One 2024 highlighted a variant in the ADAM33 gene linked to severe remodeling.
Expert Insight Tip
When writing the full article, consider quoting a pulmonologist from the 2023 ATS Guideline on Asthma to reinforce authority.
How To Spot
Clinical RedFlags
If you notice any of these, its time to ask your doctor about remodeling:
- Persistent shortness of breath even after a rescue inhaler.
- Reduced response to bronchodilators (the fixed obstruction sign).
- Frequent exacerbations despite optimal inhaled therapy.
Objective Tests
Doctors can confirm remodeling with a few tools:
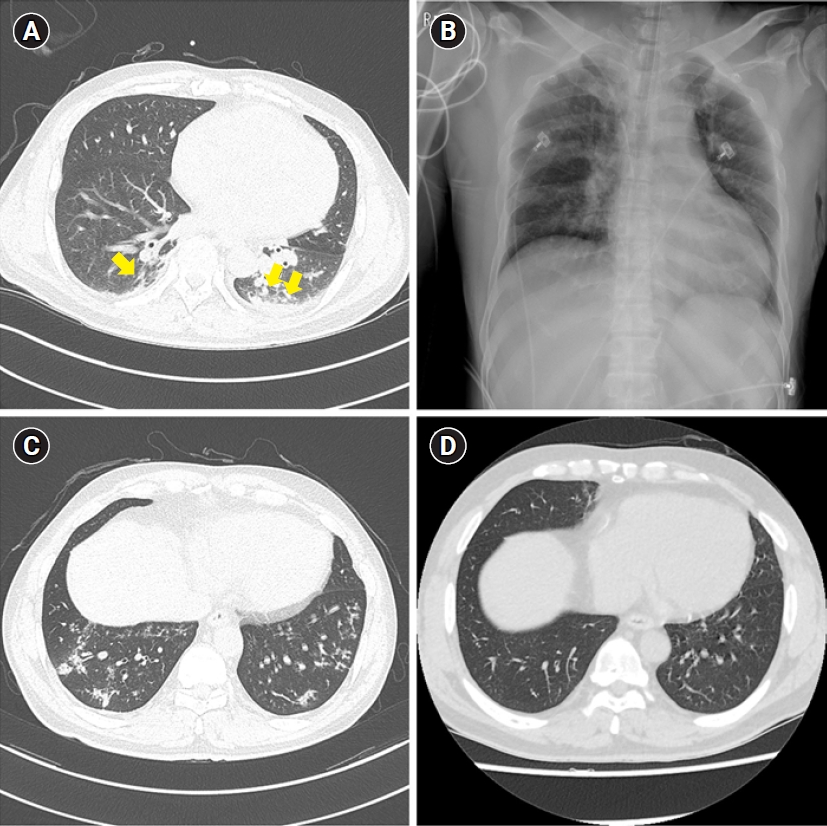
- Highresolution CT scans show wall thickness.
- Bronchial biopsies the gold standard, though rarely done.
- Impulse oscillometry detects subtle airway stiffening.
- Trend of FeNO levels high levels over years hint at ongoing inflammation that fuels remodeling.
QuickReference Table
| Test | What It Reveals | Invasiveness |
|---|---|---|
| HRCT | Wall thickness, airway lumen | Noninvasive |
| Biopsy | Fibrosis, smoothmuscle mass | Invasive |
| Oscillometry | Airway stiffness | Noninvasive |
| FeNO trend | Chronic eosinophilic inflammation | Noninvasive |
Can It Reverse
What the Evidence Says
Longitudinal studies suggest that early, aggressive therapy can halt progression and occasionally shrink the remodeled wall. A 2022 followed 150 patients on biologics for three years; about 30% showed measurable reduction in airway wall thickness.
Factors That Improve Reversibility
- Earlyintervention biologics (antiIL5, antiTSLP).
- Highdose inhaled steroids combined with longacting bronchodilators.
- Smoking cessation removes a major driver of scar tissue.
- Regular pulmonary rehab keeps the muscles flexible.
Patient Vignette
Maria, a 28yearold with mildpersistent asthma, started Dupilumab at 22. After 18months, a followup CT showed a 15% reduction in her airway wall thickness, and she could run a mile without stopping. Stories like Marias illustrate that reversible is not a mythit just needs the right timing and treatment.
Life Expectancy Impact
Mortality Data
A metaanalysis of ten cohorts published in 2023 found that the presence of remodeling increased asthmarelated mortality by roughly 12% over a decade, largely due to severe, unresponsive exacerbations.
DailyLiving Consequences
Beyond mortality, remodeling can chip away at quality of life: lower exercise tolerance, nighttime coughing, missed workdays, and the constant anxiety of will I be able to breathe tonight?
Infographic Idea (For Full Article)
Consider creating a Day in the Life timeline showing how a person with remodeling navigates a typical dayfrom morning inhaler checks to evening peakflow tracking.
Treatment Options
AntiInflammatory Backbone
Inhaled corticosteroids remain the foundation. They dampen the cytokine storm that drives fibrosis.
Biologic Agents Targeting Remodeling Pathways
- Dupilumab (antiIL4R) blocks both IL4 and IL13 signals, curbing collagen deposition.
- Mepolizumab (antiIL5) reduces eosinophils that fuel inflammation.
- Tezepelumab (antiTSLP) upstream blocker, showing promise in early trials for reversing wall thickening.
NonPharmacologic Strategies
- Bronchial thermoplasty delivers controlled heat to reduce smoothmuscle mass.
- Pulmonary rehabilitation improves overall lung mechanics.
- Allergen immunotherapy lessens chronic immune activation.
- Chest physiotherapy is also vital, especially for individuals with mucus retention issues, as seen in cystic fibrosis; learning effective chest physiotherapy cystic fibrosis techniques can greatly enhance airway clearance and lung function.
Comparison Table
| Therapy | Mechanism | Evidence for Remodeling | Cost (US$) |
|---|---|---|---|
| ICS | Suppresses cytokines | Modest slowdown | Low |
| Dupilumab | Blocks IL4/IL13 | Reduces wall thickness (30% pts) | High |
| Mepolizumab | AntiIL5 | Limited data on remodeling | High |
| Tezepelumab | AntiTSLP | Promising early results | Very High |
| Thermoplasty | Thermal reduction of muscle | Improves airflow, mixed remodeling data | Very High |
COPD Comparison
Similarities
Both asthma and COPD can develop airway fibrosis, smoothmuscle hypertrophy, and neovascularisation. The end resultstiff, narrowed airwaysis alike.
Key Differences
- Distribution: Asthma remodeling is usually central (larger bronchi); COPD affects peripheral airways and is compounded by emphysema.
- Primary driver: Smoking dominates COPD, while allergic or eosinophilic inflammation dominates asthma.
- Reversibility: Asthma shows more potential for reversal with biologics; COPD changes are often permanent.
SidebySide Chart
| Aspect | Asthma | COPD |
|---|---|---|
| Location | Central airways | Peripheral airways + alveolar loss |
| Main Trigger | Allergens, eosinophils | Tobacco smoke |
| Reversibility | Possible with early therapy | Rare |
| Typical Treatment | ICS, biologics | Bronchodilators, steroids, oxygen |
Practical Tips for You
EarlyDetection Checklist
- Do you need a rescue inhaler more than twice a week?
- Is your peakflow consistently below 80% of predicted?
- Are you experiencing nighttime cough that wakes you up?
- Have you had a chest CT or specialist talk about wall thickening?
If you answered yes to any of these, schedule a conversation with your provider about airway remodeling assessments.
SelfManagement Tools
- Keep a simple peakflow diarywrite the date, time, and reading.
- Use a smartphone app (e.g., AsthmaMD) to track symptoms and medication use.
- Set medication remindersmissed doses are a fast track to remodeling.
Resource List
Reliable sources you can trust include the American Lung Association, GINA guidelines, and the . They provide printable action plans and uptodate treatment recommendations.
Conclusion
Asthma structural remodeling may sound intimidating, but knowing the what, why, and how gives you power. First, recognize that remodeling is a measurable change that can lock in airway obstruction. Second, act earlywith inhaled steroids, targeted biologics, and healthy lifestyle choicesto halt or even shrink the scar tissue. Third, stay engaged: monitor symptoms, ask for the right tests, and partner with a trusted clinician. By keeping these three pillars in mind, you can protect your lungs, improve quality of life, and maybe even extend life expectancy.
Whats your experience with asthma and airway changes? Share your story in the comments, download our free RemodelingReady Asthma Action Plan, or reach out with any questionsyoure not alone on this journey.