At first, I thought it was just a little tummy upset that would pass on its own. Then the vomiting didnt stop, the diarrhea kept coming, and I started wondering if I needed a prescription. The short answer? Most cases of gastroenteritis clear up without antibiotics, but when the culprit is a bacterial infectionor when you belong to a highrisk groupantibiotics can be a lifesaver.
Below youll find everything you need to know: when antibiotics are actually useful, which drugs doctors usually pick, how the rules differ for adults and kids, and what risks you should watch out for. Think of this as a friendly conversation over a cup of tea, with realworld examples and clear takeaways that you can act on today.
Quick Answer Summary
Do I need antibiotics for gastroenteritis?
Most mild gastroenteritis cases are viral and resolve with hydration and rest. Antibiotics are reserved for confirmed or strongly suspected bacterial infections, especially if you have a fever over 38.5C, blood in the stool, or are immunocompromised.
When should I consider medication?
- High fever (>38.5C) persisting more than 48hours
- Bloody or mucoid diarrhea
- Severe dehydration despite oral rehydration
- Underlying conditions: very young children, elderly, or people on chemotherapy
Whats the best antibiotic for gastroenteritis?
Firstline choices are usually ampicillin for drugsensitive strains and trimethoprimsulfamethoxazole when theres a penicillin allergy or resistance. For travelers with resistant E.coli, ciprofloxacin or azithromycin may be preferred.
Bacterial vs Viral
Why antibiotics only help bacterial infections
Viruses such as norovirus or rotavirus dont have the cellular machinery that antibiotics target, so taking a pill wont speed up recovery. In fact, unnecessary antibiotics can disrupt the gut microbiome and increase the risk of .
Common bacterial culprits
Think of Salmonella, Shigella, Campylobacter, and certain strains of E.coli. These bacteria can cause more intense symptoms and, in some cases, severe complications that genuinely require antimicrobial therapy.
Realworld example
When I was volunteering at a community clinic, a 7yearold boy came in with watery diarrhea, a temperature of 39C, and bright red blood in his stool. The pediatrician ordered a stool culture, which grew Shigella. He was started on an appropriate antibiotic and improved within 48hoursclear evidence that a targeted drug can change the outcome.
Preferred Antibiotic Options
Firstline agents
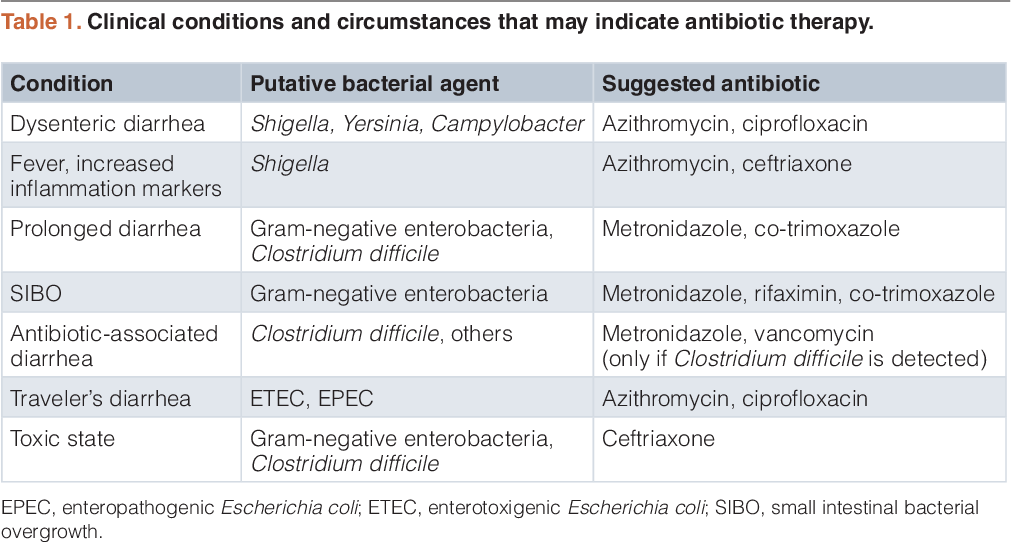
Below is a quick reference table that many clinicians use when deciding on therapy. The doses are typical for adults; pediatric dosing is weightbased and appears later.
| Drug | Typical Adult Dose | Key Indications | Notes |
|---|---|---|---|
| Ampicillin | 500mg every 6h | Drugsensitive Salmonella, Shigella | Safe in pregnancy; watch for allergy |
| TrimethoprimSulfamethoxazole | 800/160mg bid | Penicillinallergy, resistant strains | Adjust for renal function |
| Ciprofloxacin | 500mg bid | Travelrelated diarrhea, resistant E.coli | May cause tendon issues; avoid in kids unless unavoidable |
| Azithromycin | 500mg daily 3days | Alternative for fluoroquinoloneresistant traveler's diarrhea | Fewer druginteraction concerns |
| Rifaximin | 550mg tid | Noninvasive travelers diarrhea | Limited systemic absorption; not firstline for children |
When amoxicillin is considered
Amoxicillin can be effective for certain bacterial stomach infections, but only when the pathogen is known to be susceptible. Its NOT the goto drug for most gastroenteritis cases because resistance rates are high.
Guidelines snapshot
According to the , empiric therapy should be guided by local resistance patterns and patient risk factors. In plain English: doctors look at what bugs are common in your area and whether you have conditions that make infection more dangerous.
Adults vs Children
Adult dosing and considerations
Adults typically receive fixed doses (as shown in the table). Always check kidney and liver function before starting therapy, especially with drugs like trimethoprimsulfamethoxazole that are cleared renally.
Pediatric dosing basics
Kids get doses calculated by weightusually milligrams per kilogram. For example, ampicillin is often given at 50mg/kg/day divided every 6hours. A 12kg child would receive about 300mg per dose.
Special warnings for children
- Avoid tetracyclines in children under 8years (risk of teeth staining).
- Be cautious with fluoroquinolones unless absolutely necessary; theyve been linked to cartilage problems in animal studies.
- Watch for signs of dehydration earlychildren can lose fluids quickly.
Anecdote from a pediatrician
Dr. Maya Patel once told me about a toddler who was mistakenly given a full adult dose of azithromycin. The child experienced mild stomach upset, but the error highlighted how crucial weightbased calculations are. Doublecheck the scales, she says, and never assume one size fits all.
Risks & Side Effects
Common adverse reactions
Most antibiotics can cause mild gastrointestinal upsetcramping, nausea, or a change in bowel habits. The biggest red flag is , which can turn a simple bout of diarrhea into a serious, lifethreatening condition.
Allergic reactions
If you notice a rash, swelling, or difficulty breathing after a dose, stop the medication and seek emergency care. Penicillin allergies are common; thats why trimethoprimsulfamethoxazole or macrolides are useful alternatives.
Antibiotic resistance
Every time we use an antibiotic unnecessarily, we give bacteria a chance to develop resistance. Thats why doctors follow strict antibiotic stewardship rulesonly prescribe when the benefits clearly outweigh the risks.
Managing side effects
- Take the drug with food if it irritates your stomach (unless the label says otherwise).
- Consider a probiotic supplement to help keep your gut flora balanced.
- Stay hydratedfluids help flush the medication and any residual toxins.
Official Treatment Guidelines
Key recommendations worldwide
Both the World Health Organization and the American College of Gastroenterology stress that antibiotics should be reserved for:
- Confirmed bacterial pathogens (via stool culture or PCR)
- Patients with severe systemic signs (high fever, hypotension)
- Highrisk groups (infants, elderly, immunocompromised)
Quickreference chart
| Situation | FirstLine Drug | Alternative | Duration |
|---|---|---|---|
| Drugsensitive Salmonella | Ampicillin | TrimethoprimSulfamethoxazole | 57days |
| Penicillin allergy | TrimethoprimSulfamethoxazole | Azithromycin | 5days |
| Travelers diarrhea (E.coli) | Ciprofloxacin | Rifaximin | 3days |
| Severe shigellosis | Ciprofloxacin | Ampicillin | 35days |
Where to find the full guidelines
The complete is free to download, and many hospitals host their own local versions based on regional resistance patterns.
Practical Takeaway Tips
What to do at home before seeing a doctor
- Start oral rehydration solutions (ORS) 1liter of clean water with 6teaspoons of sugar and half a teaspoon of salt.
- Follow the BRAT diet (Bananas, Rice, Applesauce, Toast) only for the first few hours; resume a balanced diet as soon as you can.
- Keep a symptom diary: temperature, stool consistency, any blood, and fluid intake.
Questions to ask your healthcare provider
- Do my symptoms suggest a bacterial cause?
- Should I have a stool culture or rapid PCR test?
- If an antibiotic is needed, which one is best for my age and health status?
- What sideeffects should I monitor?
Downloadable tool
Consider using a simple Gastroenteritis Symptom Tracker (you can create one in a spreadsheet) to log the above details. It makes the conversation with your clinician much smoother and helps you spot patterns early.
Wrapping Up
In a nutshell, antibiotics are not a magic bullet for every upset stomach. They shine when youre dealing with a confirmed bacterial infection or when you belong to a vulnerable group. Choosing the right drugampicillin or trimethoprimsulfamethoxazole for most cases, ciprofloxacin or azithromycin for travelrelated concernsrequires a blend of medical expertise and awareness of local resistance trends.
Remember to stay hydrated, monitor your symptoms, and reach out to a healthcare professional if you notice redflag signs. By using antibiotics responsibly, you protect yourself and help keep these lifesaving medicines effective for everyone.
Whats been your experience with gastroenteritis? Have you ever been prescribed an antibiotic, or did you manage it at home? Share your story in the commentsId love to hear how you navigated the journey.
FAQs
When should antibiotics be prescribed for gastroenteritis?
Antibiotics are indicated when there is a confirmed or strongly suspected bacterial cause, especially with high fever, blood in stool, severe dehydration, or in high‑risk patients such as the very young, elderly, or immunocompromised.
What are the first‑line antibiotics for bacterial gastroenteritis?
Common first‑line agents include ampicillin (for drug‑sensitive strains), trimethoprim‑sulfamethoxazole (penicillin‑allergy or resistant strains), ciprofloxacin (travel‑related resistant E. coli), azithromycin (fluoroquinolone‑resistant cases), and rifaximin for non‑invasive traveler’s diarrhea.
How does antibiotic dosing differ between adults and children?
Adults receive fixed doses (e.g., ampicillin 500 mg every 6 h). Children are dosed by weight, typically in mg/kg divided throughout the day—for example, ampicillin 50 mg/kg/day divided q6h.
What are the main risks of using antibiotics for gastroenteritis?
Potential side effects include gastrointestinal upset, allergic reactions, and the serious risk of Clostridioides difficile infection. Overuse also contributes to antibiotic resistance.
Can probiotics help while taking antibiotics for gastroenteritis?
Yes, probiotic supplements may help maintain a healthy gut microbiome and reduce antibiotic‑associated diarrhea, but they should be taken a few hours apart from the antibiotic to avoid interference.