Most people dont realize that ankylosing spondylitis (AS) and scoliosis can look alike on an Xray, but they are actually two very different beasts. One is an autoimmune inflammation that can fuse the spine, the other is a sideways curvature that usually shows up in childhood.
Why does that matter? Because mixing them up can delay the right treatment, keep you in pain longer, and even affect how you move years down the road. Lets cut through the jargon and get you the clear, friendly guide you need to tell them apart and take charge of your health.
What Is Ankylosing Spondylitis
Definition & Classification
AS is a type of spondyloarthropathy basically a family of disorders where the immune system decides to attack the joints of the spine and pelvis. The hallmark is inflammation of the sacroiliac joints (the backbonetopelvis connection). Over time, that inflammation can cause the vertebrae to fuse together, turning a flexible spine into a rigid rod.
Typical Symptoms (Including Women)
The classic sign is a dull, aching pain in the lower back that gets worse after youve been still for a while (think watching TV or sitting at a desk) and improves once you start moving. Stiffness in the morning that eases after a short walk is another red flag. Women often experience a slightly different picture they might feel more peripheral joint pain or fatigue, which can make the diagnosis trickier.
How Doctors Diagnose It
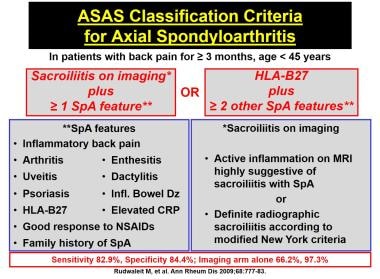
The road to an usually starts with a detailed history and physical exam, followed by imaging. An MRI of the sacroiliac joints can spot inflammation early, even before an Xray shows damage. Blood tests for the HLAB27 gene and markers like ESR or CRP add extra clues, but theyre not decisive on their own. For patients aiming for ankylosing spondylitis remission, early and accurate diagnosis is especially important to guide treatment choices.
Expert Insight Box
We see a lot of younger patients who think its just bad posture, when its actually the beginning of a chronic inflammatory process, says Dr. Laura Chen, a rheumatologist at the National Spine Center.
What Is Scoliosis
Definition & Types
Scoliosis is a lateral (sidetoside) curvature of the spine that measures more than 10 on a standing Xray. It isnt a disease by itself; its a description of a shape. The most common form is idiopathic scoliosis, where we simply dont know the cause. Secondary scoliosis can arise from neuromuscular conditions, congenital vertebral malformations, or yes from other spine diseases like AS.
Who Gets It and How It Feels
Most cases pop up during the teenage growth spurt thats why youll often hear adolescent idiopathic scoliosis. Adults can develop or worsen a curve, especially if a childhood curve was missed. Many people with mild scoliosis feel no pain at all; the curve is usually discovered during a routine school screening or a sports physical.
How Its Checked
The first step is a physical exam the Adams forward bend test, where the doctor looks for asymmetry in the rib cage. If something looks off, a standing Xray is taken to measure the Cobb angle, which tells us how severe the curve is.
RealWorld Example
Meet Alex, a 14yearold who loved basketball. During a routine checkup, his coach noticed one shoulder looked higher than the other. A quick Xray later, Alex was diagnosed with a 22 thoracic curve. Because it was caught early, a custom brace kept the curve from progressing, and Alexs game is back on track.
Can AS Cause Scoliosis
Pathophysiology Overlap
When AS inflames the front of the spine and eventually fuses the vertebrae, the natural curvature can be forced into a sideways tilt. In other words, a secondary scoliosis can appear as a byproduct of the disease. Studies have shown that around 2025% of people with longstanding AS develop some degree of scoliosis.
Clinical Evidence
A retrospective analysis published in compared 150 AS patients with 150 controls and found a statistically significant higher incidence of a lateral curvature in the AS group. The average Cobb angle for those secondary curves was modest (1218), but they still mattered for posture and comfort.
Patient Story
Maria, a 32yearold graphic designer, was diagnosed with AS at 28 after months of stiff back pain. By the time she was on medication, she noticed her left shoulder creeping forward. An Xray confirmed a 15 lumbar curve a classic case of ASinduced scoliosis. Her treatment plan was tweaked to include targeted physiotherapy, which helped keep the curve from worsening.
Key Differences Overview
| Feature | Ankylosing Spondylitis | Scoliosis |
|---|---|---|
| Root Cause | Autoimmune inflammation (often HLAB27) | Structural curvature; usually idiopathic |
| Typical Onset | Late teensearly 30s | Early adolescence (1018y) |
| Primary Curve Direction | Sagittal (forwardbending) kyphosis | Lateral (sidetoside) |
| Pain Pattern | Morning stiffness, improves with movement | Often painless unless severe |
| ExtraSpinal Issues | Uveitis, gut inflammation, skin lesions | Rarely associated with systemic disease |
| Diagnostic Tools | MRI/CT of sacroiliac joints, HLAB27 test | Standing Xray, Cobb angle measurement |
| Treatment Goal | Control inflammation, maintain flexibility | Prevent progression, correct deformity |
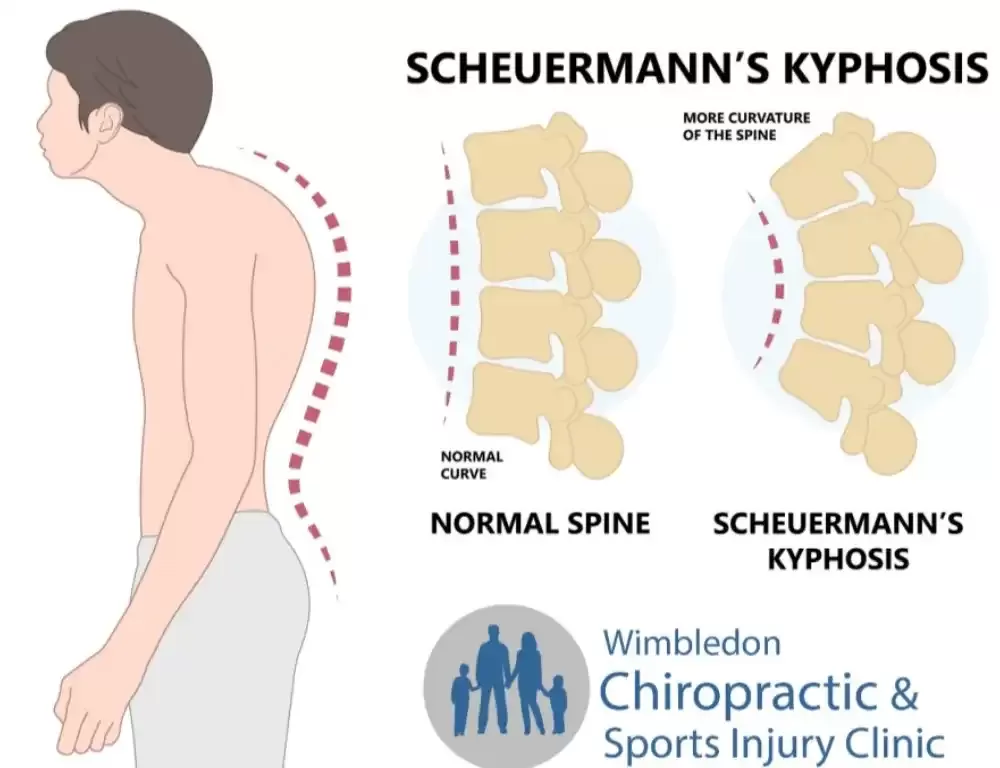
Scoliosis vs. Kyphosis
Kyphosis is an excessive forward curvature (think hunchback). While AS can cause a kyphotic posture as the spine fuses, true kyphosis is a separate alignment issue. Knowing the difference helps you target the right therapy.
Is Scoliosis an Autoimmune Disease?
Short answer: No. Scoliosis itself isnt driven by the immune system. However, secondary scoliosis can show up in autoimmune conditions like AS, which is why the two sometimes get tangled together in conversations.
Treatment Options Compared
Managing Ankylosing Spondylitis
Firstline care usually starts with NSAIDs (ibuprofen, naproxen) to tame inflammation. If pain persists, biologic drugs that block TNF or IL17 (such as etanercept or secukinumab) are gamechangers. Physical therapy isnt optional daily stretching, breathing exercises, and posture drills keep the spine from locking up. In rare, severe cases, surgeons may perform a spinal osteotomy to correct a fixed bend. Patients and clinicians often use agreed-upon AS remission criteria to judge treatment success and decide when to taper or change therapy.
Addressing Scoliosis
For curves under 25, doctors often just monitor the situation with periodic Xrays. Between 2540, a customfitted brace (like a TLSO) can halt progression, especially while the child is still growing. When the curve cracks 45 or more, surgical options such as posterior spinal fusion or growing rods (for younger kids) become the norm.
When Both Conditions CoExist
Imagine juggling a medication schedule for AS while also needing to wear a brace for scoliosis. It can feel overwhelming, but a coordinated team of rheumatologists, orthopedic spine surgeons, and physiotherapists can create a unified plan. For instance, antiinflammatory meds keep the AS flareups down, while targeted physiotherapy addresses the asymmetric forces that might worsen the scoliosis.
Expert Guidance
According to a recent guideline from the , early use of biologics paired with regular exercise yields the best longterm outcomes for AS patients, even those who develop secondary scoliosis.
Lifestyle Tips & Support
Everyday Exercise
Gentle, lowimpact activities keep the spine supple without overloading inflamed joints. Swimming, walking, and yoga are all favorites among patients. Even a 10minute daily stretch routine can make a huge difference in morning stiffness.
Posture Hacks
Use a lumbar roll or an ergonomic chair when youre at a desk. Keep screens at eye level so youre not constantly looking down. Small adjustments add up to less strain on both the spine and the surrounding muscles.
Track Your Symptoms
Consider a simple journal: note the time of day you feel stiff, any flareups, the meds you took, and what activities you did. Over weeks, patterns emerge, and youll be better equipped to discuss specifics with your doctor.
Find Community
Connecting with others who get it can lift the emotional weight. The Spondylitis Association of America and the Scoliosis Research Society both host online forums where you can swap brace tips, ask medication questions, and celebrate milestones.
MindBody Balance
Stress can amplify inflammation, so techniques like deepbreathing, meditation, or even a short daily gratitude practice can indirectly ease your physical symptoms. Remember, healing is as much about mental resilience as it is about pills and braces.
Wrapping Up Insights
At the end of the day, ankylosing spondylitis and scoliosis may share some visual similarities, but they stem from entirely different origins one autoimmune, the other structural. Understanding those roots helps you choose the right doctor, the right treatment, and the right everyday habits. If youve spotted any of the redflag symptoms we discussed, dont wait; reach out to a specialist, get the appropriate imaging, and start a conversation about your personalized care plan.
Weve covered the science, the numbers, and even some reallife stories, but the most powerful tool you have is curiosity. Keep asking questions, stay active, and lean on the community around you. Your spine and your future deserve that thoughtful attention.
FAQs
What are the main symptoms of ankylosing spondylitis vs scoliosis?
Ankylosing spondylitis often causes chronic lower‑back pain, morning stiffness that improves with movement, and possible fatigue. Scoliosis usually presents as a visible sideways curvature; many people feel no pain unless the curve is severe.
How is ankylosing spondylitis diagnosed compared to scoliosis?
AS diagnosis relies on medical history, physical exam, MRI or X‑ray of the sacroiliac joints, and sometimes HLA‑B27 blood testing. Scoliosis is identified through a physical exam (Adam’s forward bend) followed by a standing X‑ray to measure the Cobb angle.
Can ankylosing spondylitis cause scoliosis?
Yes. Long‑standing inflammation and fusion from AS can force the spine into a secondary lateral curvature. About 20‑25 % of people with advanced AS develop a mild scoliosis.
What treatment options differ between ankylosing spondylitis and scoliosis?
AS is managed with NSAIDs, biologic agents (TNF‑α or IL‑17 inhibitors), and regular physiotherapy. Scoliosis treatment depends on curve size: monitoring, bracing for moderate curves, or surgical fusion for severe curves.
When should I see a specialist for these conditions?
If you experience persistent back pain and stiffness lasting more than a few weeks, or notice an uneven shoulder or rib cage, schedule an appointment with a rheumatologist (for AS) or an orthopedic spine specialist (for scoliosis) promptly.