Ever found yourself wrestling with the question, Does this patient really meet the ASAS definition for ankylosing spondylitis? You're not alone. The answer can be crystal clear in just a few minutes if you know the right checklist. Below is a friendly walkthrough of the ankylosing spondylitis criteria ASAS, how they compare to the modified New York criteria, and a few real-world tips that keep you from getting tangled in jargon.
What Are ASAS?
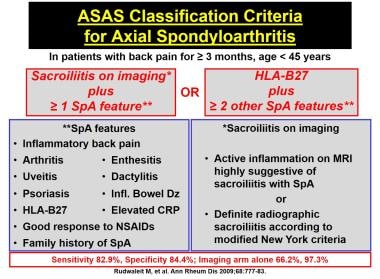
First off, ASAS stands for the Assessment of SpondyloArthritis International Society. Back in 2011 the group published a two-arm classification that was meant to catch patients earlier than the old Modified New York criteria could. The idea? Split the diagnosis into an imaging arm and a clinical arm so that doctors can still label axial disease even when X-rays look normal.
Imaging Arm Basics
If you have a sacroiliac MRI that shows active inflammation (bone marrow edema) or definitive structural changes, you've already crossed the first line. In plain language, the MRI needs to light up like a neon sign in the sacroiliac joints. That's the ASAS criteria MRI component.
Clinical Arm Essentials
When the MRI is inconclusive, the clinical arm steps in. You need:
- Back pain that started before age 45
- At least1 of the following:
- Inflammatory back pain (improvement with exercise, nighttime awakening)
- HLAB27 positivity
- Good response to NSAIDs
- Family history of spondyloarthritis
- Other extraarticular features (uveitis, psoriasis, IBD)
This two-pronged setup is what the ASAS criteria for inflammatory back pain revolves around a neat way to catch disease that would otherwise slip under the radar.
Applying ASAS Criteria
Knowing the rules is half the battle; using them in a busy clinic is the other half. Let's break it down into a workflow you can actually follow while the coffee brews.
Step-by-Step: Imaging Arm
- Order a sacroiliac MRI with short-tau inversion recovery (STIR) sequences they highlight the edema we need.
- Ask the radiologist to specifically look for bone marrow edema or erosions in both SI joints.
- If the report mentions active sacroiliitis, you can immediately apply the ASAS classification.
Step-by-Step: Clinical Arm
- Screen every patient with chronic back pain for age-of-onset (<45 years).
- Run through the five clinical features (inflammatory back pain, HLAB27, NSAID response, family history, extraarticular signs).
- Count the positives you need at least one, plus the age criterion, to meet the clinical arm.
Need a quick calculator? The AS remission criteria tool does the heavy lifting for you.
Documentation Tips
Insurance folks love numbers. Put the exact clinical criteria you used in the note, attach the MRI images, and flag HLAB27 results. That way, you've got a solid paper trail for both research registries and billing.
ASAS vs Others
Now you might wonder, If ASAS is so great, why do we still hear about the Modified New York or even the AMOR criteria? Each system has its own vibe.
Key Differences at a Glance
| Feature | ASAS (2011) | Modified New York (1984) | AMOR (2020) |
|---|---|---|---|
| Age limit | 45yr (back pain) | No age limit | 50yr |
| Imaging required | MRI + X-ray | Plain X-ray only | MRI + clinical |
| Sensitivity (early disease) | ~82% | ~55% | ~78% |
| Specificity | ~86% | ~91% | ~84% |
What does this mean for you? In early-stage disease, the ASAS criteria capture almost twice as many patients as the Modified New York system. The AMOR criteria sit somewhere in the middle, offering a compromise when MRI isn't readily available.
Peripheral ASAS Criteria
Not all spondyloarthritis shows up in the spine. The ASAS criteria for peripheral spondyloarthritis let you diagnose patients with arthritis, enthesitis, or dactylitis even when the back is quiet.
When Back Pain Is Absent
Here's the short list to remember:
- One or more peripheral joint or enthesial inflammation.
- At least one additional SpA feature (like uveitis, psoriasis, IBD, HLAB27, or a positive family history).
- Imaging of the affected site showing inflammation (you can use MRI, ultrasound, or even plain X-ray if it shows erosions).
Think of it as the friend-of-the-spine pathway useful for rheumatologists who see a lot of hand or foot complaints.
Extra-Articular Features
Uveitis, psoriasis, and inflammatory bowel disease are the classic sidekicks that can tip the scales. When you spot any of these, the peripheral ASAS criteria become even more convincing.
Common Pitfalls
Even seasoned clinicians stumble. Let's call out a few myths that keep cropping up.
Myth: Only X-ray Can Confirm Ankylosing Spondylitis.
That's a relic from the pre-MRI era. X-rays are great for chronic changes, but the modern ASAS criteria MRI component catches inflammation months before you see any bony fusion.
Pitfall: Relying on One Positive MRI Finding
Not every bone marrow edema equals sacroiliitis. Look for the typical distribution (subchondral, symmetric) and pair it with clinical features. A lone spot of edema in a trauma patient could be a false-positive.
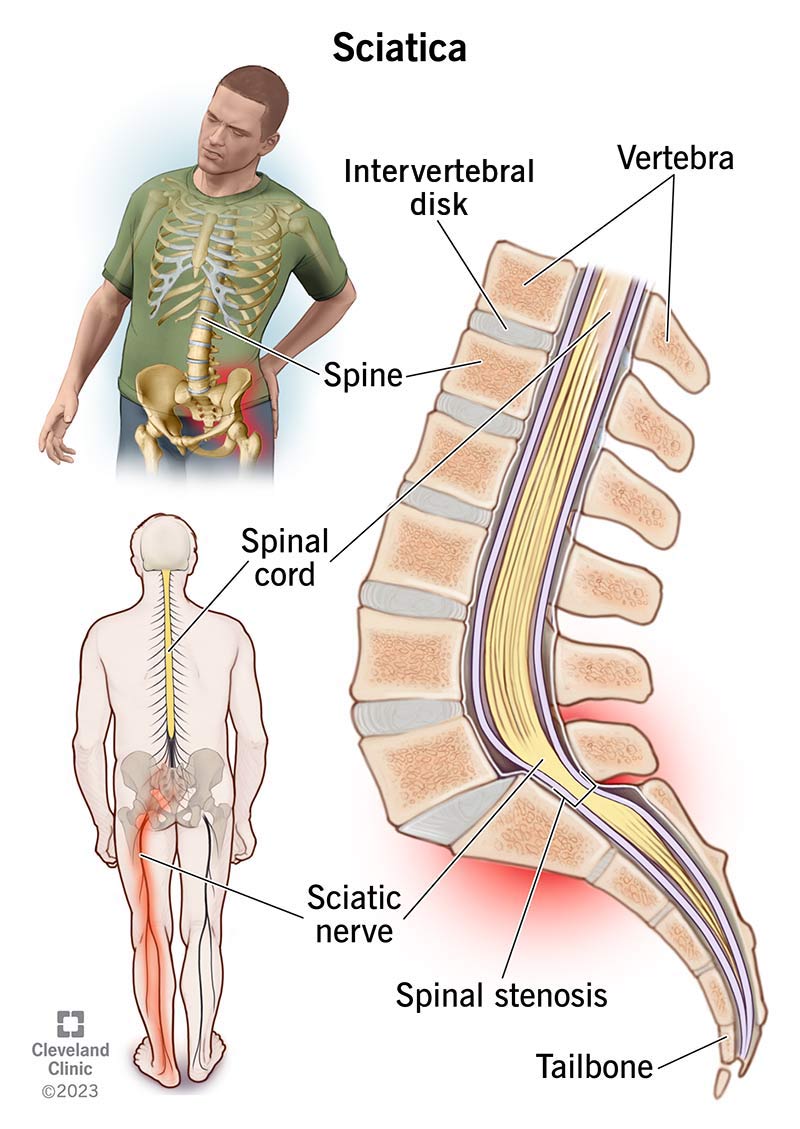
Risk: Mistaking Mechanical Back Pain for Axial SpA
Degenerative disc disease can mimic inflammatory pain, especially in older adults. The age cutoff (<45yr) and the hallmark of morning stiffness that improves with exercise are your safety nets.
Quick Red-Flag Checklist
- Age >45 and isolated mechanical pain think degenerative disease.
- Positive MRI but no clinical features reevaluate imaging protocol.
- Persistent NSAID response without other features consider other musculoskeletal disorders.
ASAS Latest Updates
Science never sleeps, and the ASAS guidelines have been fine-tuned over the past few years.
2022 ASAS-EULAR Recommendations
The latest European League Against Rheumatism (EULAR) paper stresses early MRI, a stricter definition of inflammatory back pain, and the inclusion of patient-reported outcome measures. In practice, that means you should order an SI-joint MRI as soon as the clinical arm is suspected, not after months of trial-and-error.
D2M axSpA From Diagnosis to Management
A 2024 study introduced the D2M axSpA concept, linking early diagnosis (the D) with a fast-track treatment window (M). The takeaway? The sooner you apply the ASAS criteria, the sooner patients can start biologics, dramatically improving long-term function and increasing chances of ankylosing spondylitis remission.
Practical Tools for Busy Clinicians
Beyond the MDCalc link above, the official ASAS handbook (PDF) is freely downloadable from the society's website. It includes the full algorithm, imaging protocols, and even a handy quick-look chart you can print for the exam room.
Putting It All Together
Here's a condensed cheatsheet you can keep on your phone or sticky note:
- Patient <45yr with chronic back pain? Check for inflammatory features.
- Positive HLAB27, family history, or extraarticular signs? You're halfway there.
- Order SI-joint MRI with STIR sequence look for bone marrow edema.
- If MRI positive ASAS classification met. If MRI negative apply clinical arm.
- Document every criterion; use the AS remission criteria for quick validation.
Remember, the goal isn't to tick boxes for an algorithm but to offer patients a clear, compassionate pathway to diagnosis and treatment. When you combine the science of the ASAS criteria with a listening ear, you turn a confusing health puzzle into a solvable story.
FAQs
What are the two arms of the ASAS criteria?
The ASAS classification has an imaging arm (positive sacro‑iliac MRI or X‑ray) and a clinical arm (back pain <45 yr plus ≥1 SpA feature such as inflammatory pain, HLA‑B27, NSAID response, family history, or extra‑articular manifestations).
When can I use the clinical arm without an MRI?
If the patient’s MRI is normal or unavailable, you can still meet the ASAS classification by fulfilling the clinical arm requirements: age‑of‑onset <45 yr, chronic back pain, and at least one additional SpA feature.
How does the ASAS criteria differ from the Modified New York criteria?
Modified New York relies on plain‑film sacroiliitis plus limited clinical signs, making it less sensitive early on. ASAS incorporates MRI and a broader set of clinical features, capturing disease up to 30 % earlier.
Can the ASAS criteria be applied to peripheral spondyloarthritis?
Yes. The peripheral ASAS criteria diagnose patients with peripheral arthritis, enthesitis, or dactylitis when they have at least one SpA feature (e.g., uveitis, psoriasis, IBD, HLA‑B27) and imaging evidence of inflammation at the affected site.
What are common pitfalls when interpreting a sacroiliac MRI for ASAS?
False‑positives can occur from isolated bone‑marrow edema due to trauma or infection. Look for typical subchondral, symmetric lesions and always correlate with clinical features before confirming sacroiliitis.