Lets get straight to the point: if you or someone you love has heart failure, chances are irondeficiency anemia could be silently aggravating everythingfrom fatigue to frequent hospital visits. Treating that anemiausually with an IV iron infusioncan lift energy levels, shrink breathlessness, and even lower the risk of another heart failure flareup. Its not a miracle cure, but its a proven, evidencebacked way to feel better and stay out of the ER.
Why does this matter? Because the combination of heart failure and anemia is common yet often missed, and the right treatment can make a real difference in daily life. Below, Ill walk you through the why, the how, and the whatifs, all in a friendly, nojargon stylejust a chat between friends.
Why Heart Failure Causes Anemia
First, lets unpack why a failing heart can steal iron from the body. Its not magic; its biology.
What is anemia in heart failure?
Anemia in heart failure (HF) is a drop in red blood cells or hemoglobin that makes the blood less able to carry oxygen. About onethird of people with chronic HF also have anemia, and this combo worsens symptoms and shortens survival.
Pathophysiology: iron loss, reduced absorption, inflammation
Your hearts reduced pumping power means less blood reaches the kidneys and gut. The kidneys produce less erythropoietina hormone that tells bone marrow to make red cells. Meanwhile, chronic inflammation in HF raises hepcidin, a protein that blocks iron absorption from food and traps iron inside storage cells. The result? Both absolute (real iron shortage) and functional (iron locked away) iron deficiency.
Quick Fact Box 5 Ways Heart Failure Steals Iron
- Poor gut perfusion less iron uptake
- Elevated hepcidin iron blocked in cells
- Renal hypoperfusion less erythropoietin
- Frequent diuretic use iron lost in urine
- Inflammatory cytokines bonemarrow suppression
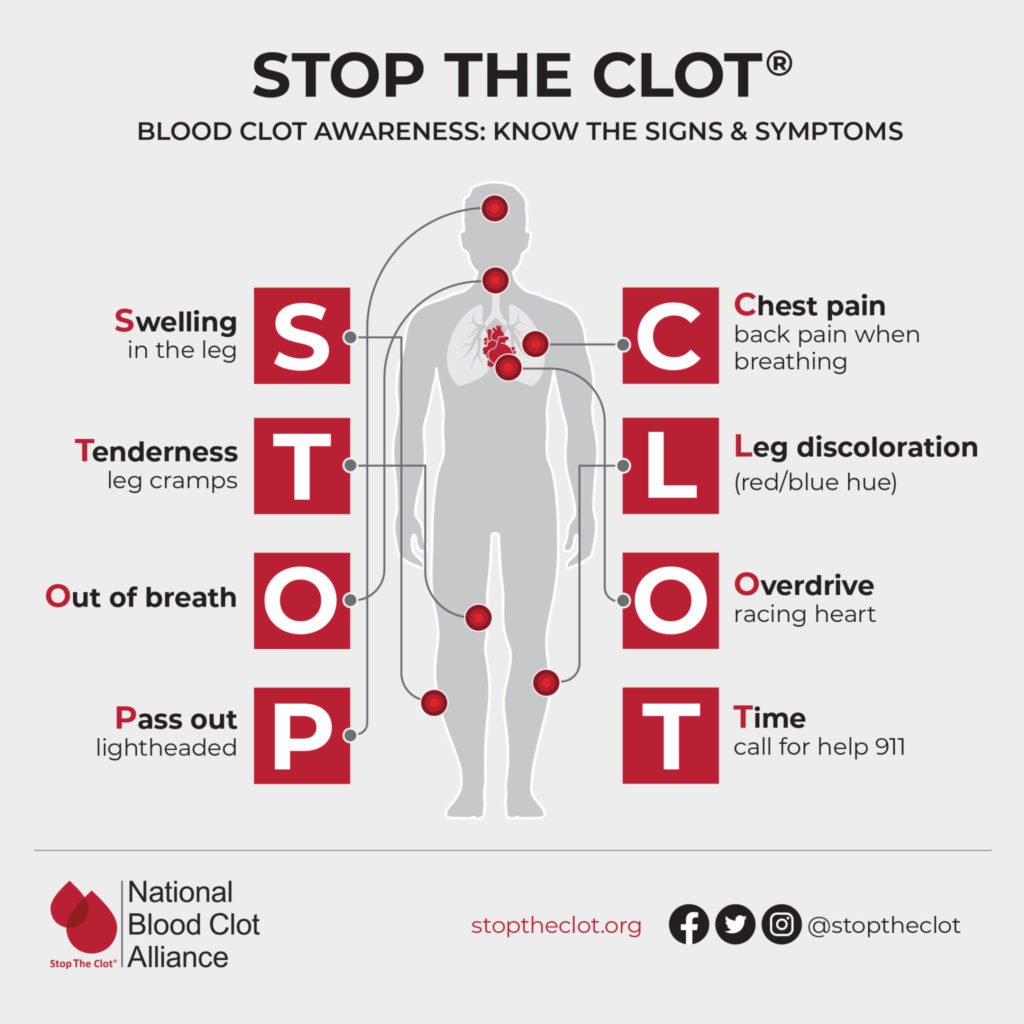
Signs of anemic heart failure
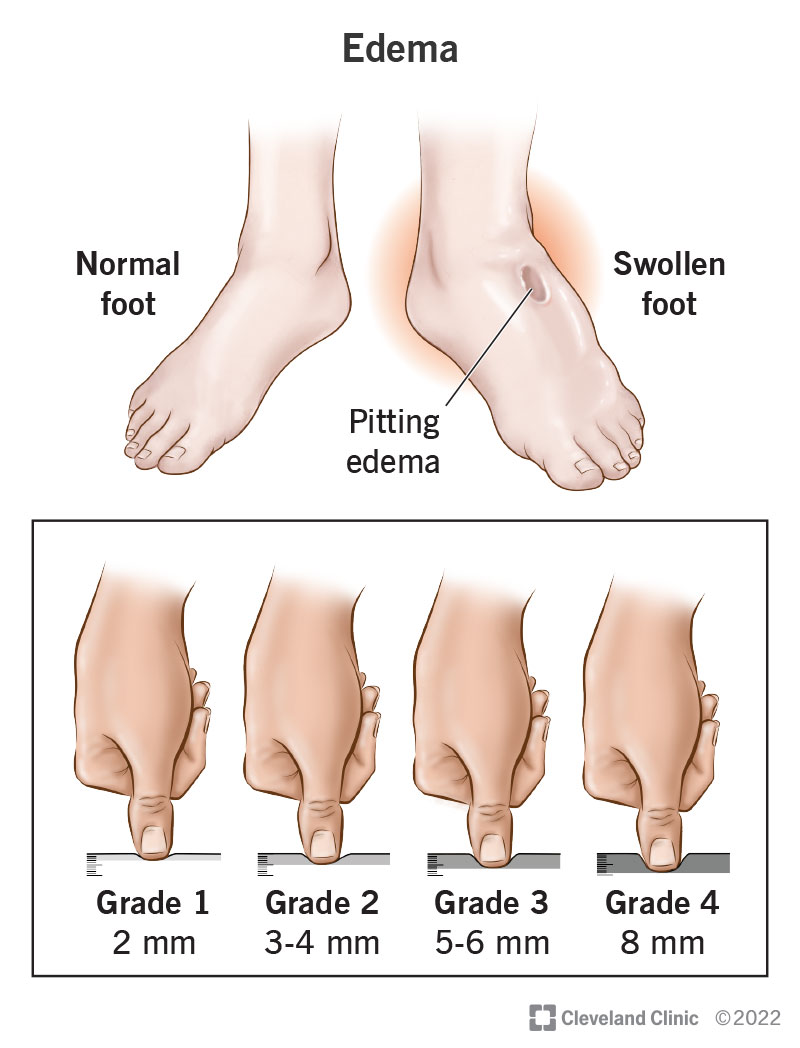
Symptoms often overlap, making it tricky to spot. Look for:
- Unexplained fatigue or weakness
- Shortness of breath on mild exertion
- Palpitations or rapid heartbeat
- Pale skin, especially on lips and nail beds
- Reduced exercise tolerance (you notice you cant walk the same distance as before)
Diagnosing Anemia in Heart Failure
Lab thresholds & when to test
Guidelines suggest checking hemoglobin (Hb) at every HF clinic visit. For men, Hb<13g/dL; for women, Hb<12g/dL usually flags anemia. Ferritin <100g/L or transferrin saturation (TSAT) <20% points to iron deficiency, even if Hb is borderline.
Differentiating absolute vs. functional iron deficiency
Absolute iron deficiency means total body iron stores are low (low ferritin). Functional deficiency means total stores may be normal but iron isnt available for redcell production (low TSAT, high ferritin). Treatment is similarIV iron works for both.
Comparison Table Lab Cutoffs
| Parameter | Cutoff | Interpretation |
|---|---|---|
| Hemoglobin | <13g/dL (men) / <12g/dL (women) | Anemia |
| Ferritin | <100g/L | Absolute iron deficiency |
| Ferritin | 100300g/L + TSAT <20% | Functional iron deficiency |
| TSAT | <20% | Iron not available for erythropoiesis |
When to suspect hidden anemia
Even a grayzone Hb of 1213g/dL can hide clinically relevant iron deficiency, especially if the patient feels unusually tired. In such cases, ordering ferritin and TSAT is wise.
EvidenceBased Treatment Options
Intravenous Iron the cornerstone
IV iron, especially ferric carboxymaltose (FCM) or ferric derisomaltose (FD), is the gold standard. A single 1000mg infusion can raise Hb by 12g/dL and improve NYHA class in weeks.
Preferred formulations & dosage
Both FCM and FD are approved for HFrelated iron deficiency. Typically, you give:
- FCM: 1000mg total (500mg infusion, repeat after 1week if needed)
- FD: 1000mg total in one go, no repeat
Clinical outcomes
Multiple randomized trialslike the show IV iron reduces HF hospitalizations by ~30% and improves qualityoflife scores. The now recommend IV iron for any HF patient with ferritin<100g/L or TSAT<20%.
Safety profile
Serious allergic reactions are rare (<0.1%). Common side effects include mild infusion site discomfort, nausea, or transient headache. Monitoring for hypotension during the first 30minutes is standard practice.
Oral Iron why it often fails
Oral tablets sound easy, but in HF theyre usually ineffective. The same inflammation that drives hepcidin also blocks gut absorption, so you end up taking a bottle of pills for weeks with little change in labs.
Blood Transfusion reserved for emergencies
Transfusions are lifesaving when Hb drops <7g/dL or the patient becomes hemodynamically unstable. However, volume overload can worsen congestion in HF, and repeated transfusions raise the risk of alloimmunisation. Use sparingly, and always pair with strategies to address the underlying iron deficiency.
ErythropoiesisStimulating Agents (ESAs)
ESAs (e.g., darbepoetin) can boost redcell production but carry risks of thromboembolic events, especially in HF patients with atrial fibrillation. Current suggest ESAs only when iron repletion fails and anemia remains severe.
Adjunct Strategies nutrition, exercise, HF meds
While IV iron does most of the heavy lifting, a balanced diet rich in heme iron (red meat, poultry) helps maintain stores. Pair it with vitaminC (citrus, bell peppers) to improve absorption. Regular, moderate exercise also stimulates erythropoiesis, and optimizing HF meds (ARNI, betablockers) can indirectly support better iron metabolism. For patients with reduced exercise tolerance due to breathlessness, an exercise stress test can help quantify functional capacity and guide safe activity plans.
Practical Implementation Steps
Stepbystep IViron protocol
Heres a simple flow you can discuss with your cardiologist:
- Screen: Check Hb, ferritin, TSAT at every 3month HF visit.
- Confirm deficiency: Ferritin<100g/L OR ferritin 100300g/L with TSAT<20%.
- Preinfusion checks: Blood pressure, allergies, baseline labs.
- Infusion: Administer 500mg FCM over 15minutes; repeat after 1week if needed to reach total 1000mg.
- Postinfusion monitoring: Observe 30minutes for hypotension or reaction.
- Followup: Recheck labs at 4weeks; repeat infusion if ferritin still <100g/L or symptoms persist.
Printable checklist (downloadable PDF)
Feel free to copy the above steps into a PDF you can hand to your providera handy way to keep the conversation focused.
Shared decisionmaking conversation starter
Try this line with your doctor: I read that IV iron can improve my energy and reduce hospital visits. Could we check my iron levels and discuss whether thats a good option for me? It shows youre engaged and opens the door for a collaborative plan.
Followup schedule & outcome tracking
Track your symptoms (fatigue score, shortness of breath) and lab values in a simple table. Seeing numbers improve over weeks is motivating and helps your clinician finetune treatment.
Balancing Risks and Benefits
Benefits summary
In short, IV iron can:
- Boost hemoglobin by 12g/dL in 46weeks
- Improve exercise capacity and NYHA class
- Cut HF rehospitalization risk by roughly onethird
- Enhance overall quality of lifemore energy for daily chores, grandchildren, or that hobby you love.
Potential risks
Every medical intervention has a downside:
- Rare allergic reactions (monitor for ~30minutes)
- Transient iron overload if dosing isnt adjustedlabs help avoid this
- Cost and insurance coverage considerations (many plans now cover FCM for HF)
Riskmitigation checklist
- Confirm iron studies before each infusion.
- Stay within guidelinerecommended total dose (max 2000mg per year).
- Report any new wheeze, rash, or dizziness immediately.
- Keep a copy of infusion records for your insurance.
Looking Ahead: Future Research
Emerging oral iron formulations
Newer oral agents encapsulated in nanoparticles aim to bypass hepcidin blockage. Early phase2 trials look promising, but theyre not yet guidelineready.
Combined ESA + IViron trials
Researchers are testing whether a lowdose ESA added to IV iron can further improve outcomes in severe anemia without increasing clot risk. Results are expected later this year.
Personalized medicine biomarkers for response
Scientists are hunting for genetic or protein markers that predict which HF patients will benefit most from iron therapy. Imagine a future where a simple blood test tells you the exact dose you need.
Conclusion
So, whats the bottom line? Anemia is a common, often hidden companion of heart failure that makes every breath feel harder. The good news is that modern IViron therapybacked by solid trials and ESC guidelinescan lift the fog, improve stamina, and keep you out of the hospital. Blood transfusions and ESAs have their place, but theyre secondary to iron repletion for most patients. By getting screened, having an open conversation with your cardiologist, and following a clear infusion protocol, you can balance the benefits and risks, and get back to the things you love.
If youve experienced anemia in heart failure, what treatment helped you the most? Share your story in the comments or reach out with questionsyoure not alone on this journey. And hey, feel free to download the checklist above and take the first step toward feeling better today.
FAQs
What causes anemia in heart failure patients?
Heart failure reduces kidney‑produced erythropoietin, raises inflammatory hepcidin, impairs gut iron absorption, and increases iron loss via diuretics, all leading to iron‑deficiency anemia.
How do doctors diagnose iron‑deficiency anemia in heart failure?
At each HF visit labs are checked: hemoglobin < 13 g/dL (men) / < 12 g/dL (women). Ferritin < 100 µg/L or ferritin 100‑300 µg/L with transferrin saturation < 20 % confirms iron deficiency.
Why is IV iron preferred over oral iron for heart failure patients?
Inflammation‑driven hepcidin blocks gut absorption, making oral tablets largely ineffective. IV iron bypasses this barrier, quickly replenishes stores and improves symptoms.
What are the risks and side effects of IV iron therapy?
Serious allergic reactions are rare (<0.1 %). Common effects include mild infusion‑site pain, nausea, headache, and a brief drop in blood pressure during the first 30 minutes.
How soon can I expect improvement after receiving IV iron treatment?
Most patients notice increased energy and reduced breathlessness within 4‑6 weeks, with hemoglobin often rising 1‑2 g/dL and a lower chance of rehospitalisation.