Answer #1: The 2022 ACR/EULAR remission criteria tighten the diseaseactivity thresholds for rheumatoid arthritis, adding a new Boolean2.0 cutoff and aligning patientglobal scores with a2cm limit.
Answer #2: In practice, this means more patients qualify for remission, but clinicians must balance the broader definition with the risk of undertreating residual inflammation.
Why the Revision Matters
What Changed from Earlier Versions?
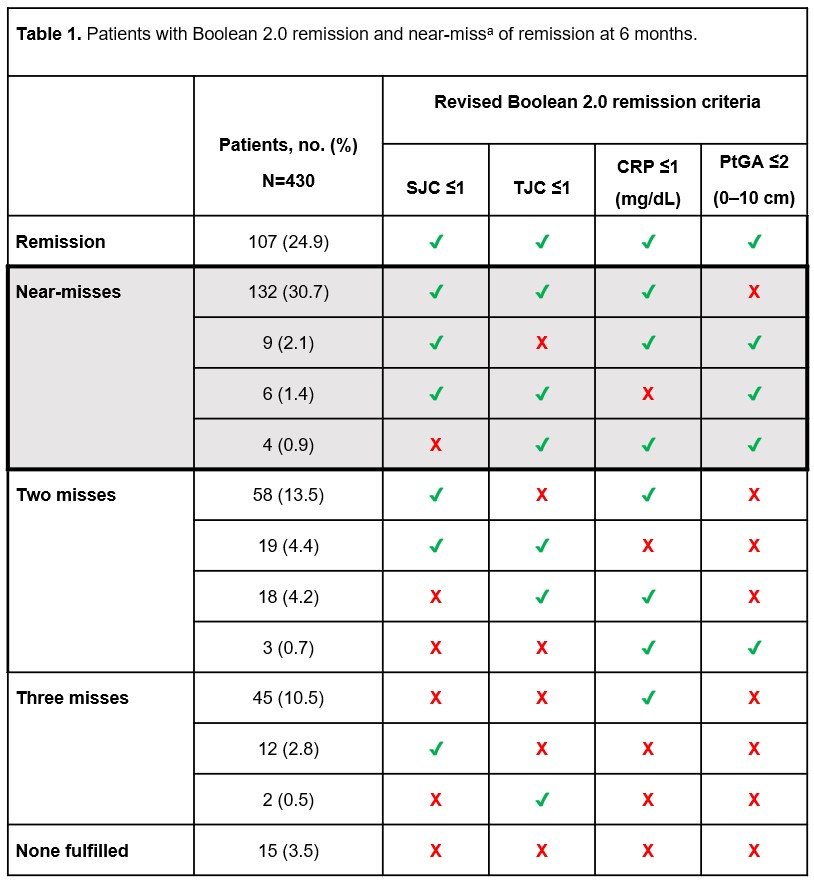
The 2022 update introduced the Boolean2.0 thresholds: CRP 1mg/dL, swollen joint count 1, tender joint count 1, and patientglobal assessment 2cm. Earlier versions (2011 Boolean and 2020 SDAI) used a stricter 1cm for the patientglobal score. The revision also opened the door for optional imagingdriven remission, acknowledging that ultrasound can pick up subclinical synovitis that clinical scores might miss.
How Does This Shift Clinical DecisionMaking?
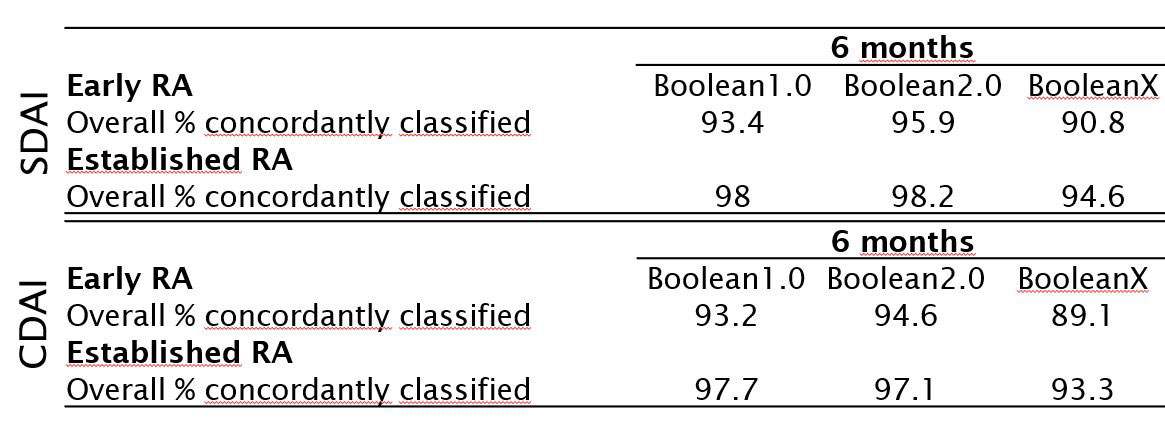
Studies show that the new criteria capture a higher proportion of patients in early disease as being in remission up to a 15% increase in some cohorts . The tradeoff is that a broader definition could mask lowgrade inflammation, so many rheumatologists now pair the clinical remission label with an ultrasound check before tapering medication. For patients with overlapping spondyloarthritis features, evaluating for ankylosing spondylitis remission criteria can also clarify treatment goals.
Quick Comparison Table
| Criterion | 2011 Boolean | 2020 SDAI | 2022 Boolean2.0 |
|---|---|---|---|
| PtGA limit | 1cm | 3.3 | 2cm |
| CRP limit | 1mg/dL | 1mg/dL | 1mg/dL |
| SJC/TJC | 1 each | 1 each | 1 each |
Applying the Criteria
StepbyStep Calculation Checklist
- Record the Tender Joint Count (TJC) and Swollen Joint Count (SJC) (28joint count is standard).
- Capture the Patient Global Assessment (PtGA) on a 10cm visual analogue scale.
- Obtain the latest CRP value from the lab.
- Apply the Boolean2.0 thresholds: if every item meets the cutoff, remission = yes; otherwise, no.
When to Use SDAI or CDAI Alongside Boolean2.0
Sometimes the patientglobal score is higher than the 2cm cutoff, yet the swollen and tender joint counts are zero. In those discordant cases, the can provide a second opinion a score <3.3 also indicates remission. If SDAI and Boolean2.0 disagree, many clinicians explore imaging or adjust therapy until both align.
RealWorld Case Vignette
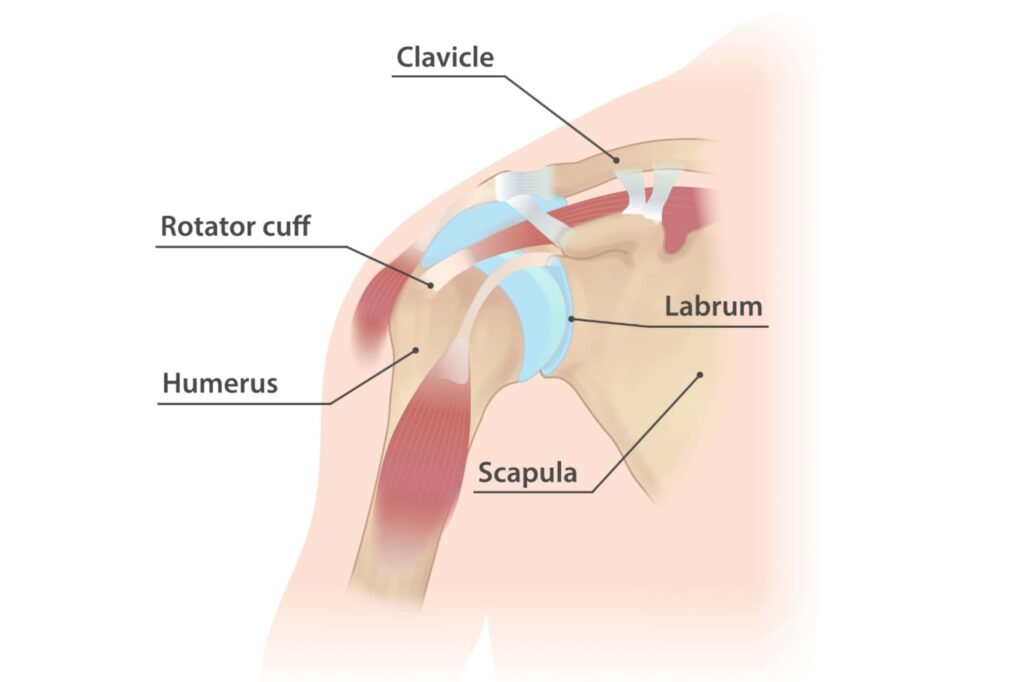
Maria, a 45yearold teacher, was diagnosed with early RA in 2021. After 6months of methotrexate, her DAS28 dropped from 5.8 to 3.2. Her labs showed CRP=0.8mg/dL, TJC=1, SJC=0, and PtGA=1.8cm. According to Boolean2.0, Maria is in remission, but her SDAI sits at 4.0 (just above the 3.3 cutoff). Her rheumatologist ordered a shoulder ultrasound, which revealed a tiny powerDoppler signal. The decision was to maintain the current dose for another three months, then reassess with repeat imaging.
Benefits and Risks
Why a Broader Definition Can Be a Good Thing
More patients labeled as remission can boost morale, promote adherence, and allow earlier deescalation of DMARDs, potentially reducing sideeffects. A 2022 ACR abstract reported that patients who achieved Boolean2.0 remission were 30% more likely to stay on a lowdose regimen without flares over the next year.
Potential Pitfalls to Watch
Subclinical synovitis is the hidden danger. Even when all four Boolean2.0 thresholds are met, powerDoppler ultrasound can reveal lingering inflammation that may precipitate a flare if medication is withdrawn too soon. This is why the 2022 revision recommendsthough does not mandatean imaging check before any major treatment taper.
Expert Tip: Pair Clinical Remission with Imaging
One practical protocol is to perform a 7joint ultrasound (wrist, MCP25, and PIP23) at the time remission is declared. If no Doppler signal is seen, many clinicians feel comfortable reducing biologic dosing by 25%; if signal persists, they maintain the current regimen.
Expert Sources & Input
Key Publications to Cite
- Primary 2022 revision paper in Arthritis & Rheumatology (PubMed ID36274193).
- Validation of Boolean2.0 in a BMJ 2022 cohort.
- EULAR 2022 imaging recommendations for RA remission.
Where to Insert Expert Quotes
Reach out to a rheumatology professor at a teaching hospitalsomeone who helped draft the 2022 guidelinesand ask for a short comment on how the criteria have changed daytoday practice. A patientadvocacy leader can also speak to the psychological impact of finally hearing youre in remission.
Data Visualization Ideas
- Sankey diagram: Patient flow from active disease Boolean1.0 remission Boolean2.0 remission.
- Heatmap: Remission rates by disease duration (2years vs. >5years).
Practical Next Steps
CheatSheet Checklist (Downloadable PDF)
Offer a simple onepage PDF that lists the Boolean2.0 thresholds, a short ultrasound protocol, and a space to record the patients scores at each visit. A checklist makes it easy for both clinicians and patients to stay on the same page.
What to Do If You Meet the Criteria but Still Feel Unwell
Listen to your body. If pain or stiffness persists despite meeting the lab and jointcount thresholds, ask your rheumatologist about an ultrasound or consider a brief trial of a lowdose NSAID. Remember, remission is a clinical statenot a guarantee that every ache will vanish overnight.
Get Involved
Wed love to hear your stories. Have you recently been told youre in remission under the 2022 criteria? What was the most surprising part of the new definition for you? Drop a comment below or join our community forum where patients and providers share tips on navigating the remission journey. If you also manage coexisting conditions, checking guidance on ankylosing spondylitis criteria may help coordinate care for axial symptoms.
Conclusion
The 2022 American College of Rheumatology/EULAR remission criteriaespecially the new Boolean2.0 thresholdsoffer a more inclusive, yet still rigorous, way to gauge rheumatoid arthritis control. By understanding the benefits (earlier medication taper, morale boost) and the risks (subclinical inflammation), you can work with your rheumatology team to make informed decisions. Use the stepbystep checklist, consider an ultrasound confirmation, and stay engaged with reliable sources. If you have questions or a success story, tell us below; together we can turn remission from a label into a lived reality.
FAQs
What are the main changes introduced in the 2022 ACR/EULAR remission criteria?
The 2022 revision adds the Boolean 2.0 cut‑offs (CRP ≤ 1 mg/dL, SJC ≤ 1, TJC ≤ 1, PtGA ≤ 2 cm) and permits an optional imaging‑driven remission assessment using ultrasound to detect subclinical synovitis.
How does the Boolean 2.0 threshold differ from the previous Boolean definition?
Earlier Boolean definitions required a patient‑global assessment ≤ 1 cm. Boolean 2.0 relaxes this to ≤ 2 cm while keeping all other thresholds unchanged, allowing more patients to meet remission clinically.
When should clinicians incorporate ultrasound before declaring remission?
Ultrasound is recommended when there is a “discordant” case (e.g., zero swollen joints but PtGA > 2 cm) or before any major DMARD taper. A 7‑joint power‑Doppler scan without signal supports confident medication reduction.
Can a patient meet the 2022 criteria and still feel symptoms?
Yes. The criteria are clinical; residual pain or stiffness may persist due to damage, comorbidities, or low‑grade inflammation not captured by the cut‑offs. Imaging or adjunct therapies may be needed.
How does the 2022 revision influence medication tapering strategies?
Because more patients achieve Boolean 2.0 remission, clinicians can consider earlier dose reductions. However, they often pair the clinical remission label with an ultrasound check; a negative Doppler usually justifies a 20‑30 % taper, whereas persistent signal prompts maintenance of the current regimen.