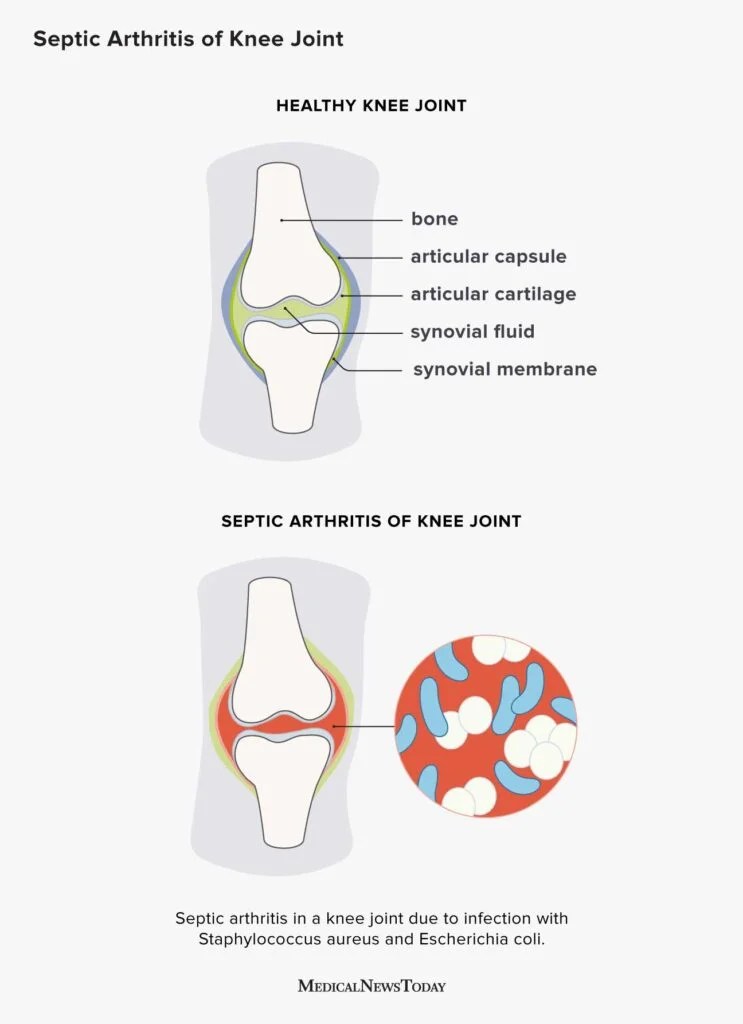
Septic arthritis happens when germs slip into a joint, most often through the bloodstream. The fastest way to spot it is sudden, severe joint pain plus swelling and fever. The main culprits are bacteria like Staphylococcus aureus and Streptococcus species, but injuries, surgeries, injections, and even skin infections can open the door. Knowing the routes and risk factors helps you act before the infection damages the joint.
Germ Entry Routes
Hematogenous Spread The Most Common Cause
When bacteria travel through the blood and lodge in a joint, thats called hematogenous spread. Its responsible for the majority of septic arthritis cases, especially in otherwise healthy people. The usual suspects are Staphylococcus aureus, followed by Streptococcus pyogenes, Streptococcus pneumoniae, and a handful of Gramnegative rods.
According to the , bacteremiathe presence of bacteria in the bloodstreamis the gateway for these microbes. Even a tiny skin scrape can seed the blood, especially if your immune system is distracted by another infection.
Direct Inoculation Injuries, Procedures, and Injections
Anything that punctures the joint can introduce germs straight into the space. Think of a deep cut over the knee, a needleguided joint aspiration, or a kneereplacement surgery. Intravenous drug use is a notorious example; contaminated needles provide a fasttrack highway for bacteria.
Realworld example: a 45yearold carpenter slipped on a nail, got a puncture wound on his ankle, and a week later woke up with a throbbing ankle joint that wouldnt bend. The doctor performed an aspiration and found a classic picture of septic arthritis caused by a skinorigin Staph infection.
Contiguous Spread Nearby Infections
Sometimes an infection thats sitting next to a joint spills over. Cellulitis, a urinarytract infection, or osteomyelitis (bone infection) can extend into the joint capsule, especially when the joint sits close to the infected tissue, such as the hip or the shoulder.
Examples of Contiguous Sources
- Cellulitis of the thigh spilling into the hip joint.
- Kidney infection reaching the sacroiliac joint.
- Dental abscesses that travel via veins to the temporomandibular joint.
Who Is At Risk
AgeRelated Vulnerability
Infants and toddlers have higher rates of bloodstream infections, making them prime candidates for hematogenous septic arthritis. On the other side of the spectrum, elderly adults often have weakened immune systems and may already have joint prostheses, which act like a welcoming mat for bacteria.
Underlying Health Conditions
Having diabetes, rheumatoid arthritis, chronic kidney disease, or being on immunosuppressive medication (like steroids or biologics) dramatically ups the odds. These conditions either impair your immune defenses or provide an environment where bacteria can thrive.
Lifestyle and Exposure Factors
Things like intravenous drug use, recent dental work, or poor wound care after a cut increase the chance of germs finding their way into a joint. Even frequent gym-goers should be mindful of scrubbeddown equipmenttiny cuts can become entry points.
Prevalence Snapshot
| Risk Factor | Approx. Prevalence in Septic Arthritis Cases |
|---|---|
| Infants & toddlers | 30% |
| Elderly (65) | 25% |
| Diabetes | 20% |
| Joint prosthesis | 15% |
| IV drug use | 10% |
Data compiled from CDC and NHS surveillance reports.
Key Warning Signs
Classic Triad: Pain, Swelling, Limited Motion
Think of a joint that suddenly feels like its been crushed, is visibly swollen, and refuses to move. The pain is often intense enough to keep you awake at night.
Systemic Clues Fever, Chills, Malaise
Because the infection is usually in the blood, youll often experience a fever (sometimes over 101F), shaking chills, and a general feeling of being under the weather.
RedFlag Locations Hip, Shoulder, Spine
Infections in deeper joints like the hip or shoulder can be especially dangerous because the infection can spread to surrounding muscles and even cause sepsis. If you notice severe, deeplying pain in those areas, consider it urgent.
QuickCheck Checklist
- Sudden, severe joint pain?
- Visible swelling or redness?
- Fever or chills?
- Reduced range of motion?
If you tick three or more, call your doctor right away. Early treatment can be the difference between full recovery and longterm joint damage.
How Diagnosis Works
Clinical Evaluation History & Physical Exam
Doctors start by asking when the pain began, any recent injuries, surgeries, or infections, and theyll gently test the joints range of motion while checking for warmth and tenderness.
Laboratory Tests
Synovial fluid analysis is the gold standard: a needle draws fluid from the joint, which is then checked for white blood cell count, Gram stain, and culture. Blood testsCBC, ESR, and CRPhelp gauge the overall inflammatory response.
Imaging Studies
Xrays show bone erosion but often look normal early on. Ultrasound can detect fluid collections, and MRI is the most sensitive for spotting early bone and softtissue involvement.
Differential Diagnosis Table
| Condition | Key Lab Findings | Typical Imaging |
|---|---|---|
| Septic Arthritis | Synovial WBC >50,000cells/L, Positive culture | Joint effusion on US; early bone edema on MRI |
| Gout | Synovial WBC 1530,000cells/L, Negative culture, Needleshaped crystals | Typical doublecontour sign on DECT |
| Rheumatoid Arthritis | RF positive, AntiCCP, Chronic elevation of ESR/CRP | Symmetrical joint space narrowing, erosions |
Standard Treatment Guidelines
Empiric Antibiotics FirstLine Agents
Because time is crucial, doctors start broadspectrum antibiotics while waiting for cultures. A common regimen includes vancomycin (covers MRSA) plus ceftriaxone (covers Gramnegative organisms). Once the specific bug is identified, therapy narrows to target it precisely.
Joint Drainage Techniques
Removing infected fluid is essential. Options range from simple needle aspiration (often done in the emergency department) to arthroscopic washout or, in severe cases, open surgical drainage.
Role of Surgery & LongTerm Antibiotics
For prosthetic joint infections or when drainage fails, surgeons may need to replace the implant. After the acute phase, patients usually complete a 46 week course of oral antibiotics, sometimes followed by a suppressive regimen if the joint remains at risk.
Treatment Algorithm
- Urgent joint aspiration send fluid for culture.
- Start empiric IV antibiotics.
- If >48hrs, assess response: repeat aspiration if still swollen.
- Switch to targeted oral antibiotics once culture results return.
- Physical therapy begins once infection is controlled.
Complications & Effects
Immediate Danger Sepsis & Organ Failure
If the bacteria spill back into the bloodstream, sepsis can develop quickly. Sepsis isnt just fever its a lifethreatening response that can lead to organ damage. According to the , early antibiotics dramatically reduce mortality risk.
Joint Destruction & Osteoarthritis
Even with prompt treatment, the inflammatory onslaught can erode cartilage. Many survivors develop chronic joint pain and secondary osteoarthritis, especially if the infection involved a weightbearing joint like the knee or hip.
Chronic Infection Recurrence Risk
People with prosthetic joints, ongoing immunosuppression, or untreated bacteremia can experience repeat episodes. Monitoring with periodic blood work and vigilant wound care are key preventive steps.
Rehabilitation Statistics
Studies from Johns Hopkins show that about 70% of patients regain nearnormal joint function after an intensive rehab program, but the remaining 30% may need longterm pain management or joint replacement.
Prevention and Action
Managing Chronic Diseases & Blood Sugar
Keeping diabetes under control, staying uptodate on rheumatoid arthritis meds, and following your physicians advice on immunosuppressants all lower infection risk.
Proper Wound Care & Sterile Injection Practices
Clean any cut promptly with soap and antiseptic, and cover it with a clean bandage. If youre receiving an injectionwhether for steroids, vaccinations, or joint aspirationensure the provider follows strict aseptic technique.
Vaccinations That Reduce Bacterial Infections
Flu and pneumococcal vaccines dont directly prevent septic arthritis, but they lower the chance of respiratory infections that can seed the bloodstream. The recommends these for adults over 65 and anyone with chronic illnesses.
When to Call a Doctor
If you notice sudden joint pain paired with fever, dont wait for it to run its course. A quick call to your primary care physician or a visit to urgent care can save your jointand potentially your life.
Conclusion
Understanding septic arthritis causes hinges on three core ideas: (1) most infections arrive via the bloodstreamthink the most common cause of septic arthritis is hematogenous spread; (2) certain peopleinfants, the elderly, diabetics, and anyone with joint implantsneed extra vigilance; (3) early actionprompt diagnosis, targeted antibiotics, and proper drainageprevents permanent joint destruction and the frightening possibility that can septic arthritis kill you? Yes, if left unchecked, it can. By staying alert to warning signs, managing underlying health conditions, and seeking care without delay, you give yourself the best shot at a full recovery.
Wed love to hear from you. Have you or a loved one faced septic arthritis? What steps helped you navigate the diagnosis and treatment? Share your story in the comments, or drop a question if anythings still unclear. Together, we can turn a scary medical term into knowledge that protects us all.
For readers interested in related joint health topics, learn more about osteoporosis physical therapy techniques that help restore mobility after serious joint infections.
FAQs
What are the most common bacteria that cause septic arthritis?
The leading culprit is Staphylococcus aureus, followed by streptococcal species such as Streptococcus pyogenes and Streptococcus pneumoniae. Gram‑negative rods can also be involved, especially in older adults or IV drug users.
How does a joint prosthesis increase the risk of septic arthritis?
Artificial joints provide a surface where bacteria can adhere and form bio‑films, making infection harder for the immune system to clear. Even a minor skin infection or transient bacteremia can seed a prosthetic joint.
Can a simple skin infection lead to septic arthritis?
Yes. Bacteria from a cut, cellulitis, or other skin infection can enter the bloodstream (bacteremia) and travel to a joint, especially if the person has other risk factors like diabetes or a compromised immune system.
Why are infants and the elderly more prone to septic arthritis?
Infants have higher rates of bloodstream infections, while elderly individuals often have weakened immunity, comorbidities, and may already have joint replacements—all of which raise susceptibility.
What should I do immediately if I suspect septic arthritis?
Seek medical attention urgently. Early joint aspiration for fluid analysis, prompt IV antibiotics, and drainage are critical to prevent permanent joint damage and life‑threatening sepsis.