Overview of Adrenal Lesions
What is an adrenal incidentaloma?
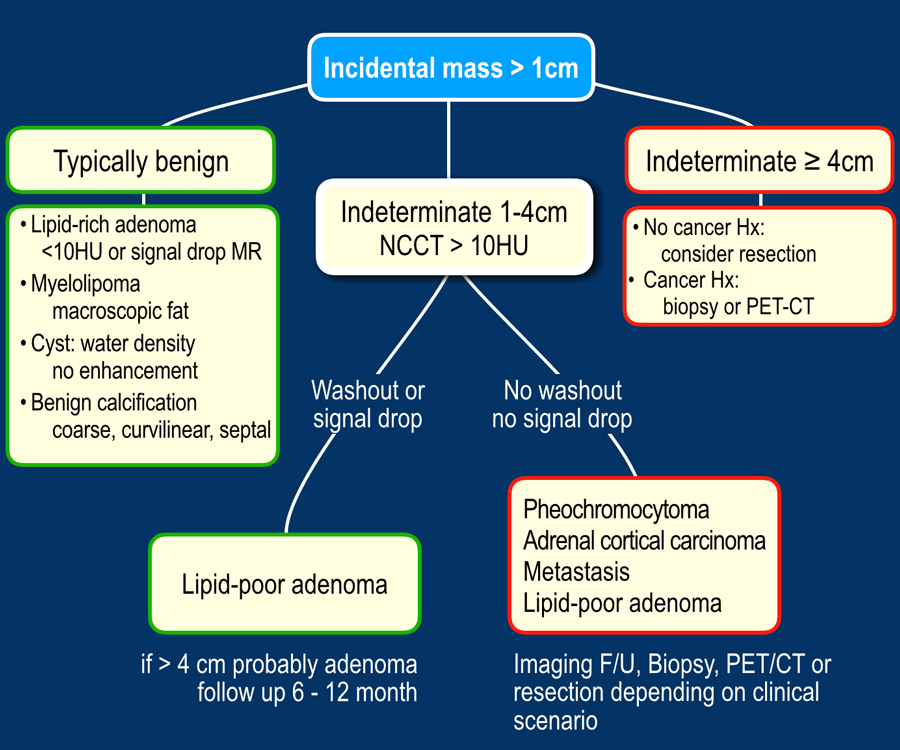
An adrenal incidentaloma is a mass >1cm discovered unintentionally on an imaging study that wasnt ordered to look at the adrenals. These foundbyaccident lesions pop up in about 5% of abdominal CTs, especially as people get older.
Why does characterizing adrenal findings matter?
Getting the nature of the lesion right can spare a patient unnecessary surgery, avoid needless hormonal testing, and focus treatment where it truly matters. On the flip side, missing a malignant lesion can delay lifesaving therapy.
Who relies on adrenal imaging?
- Radiologists interpreting the scan
- Endocrinologists evaluating hormone excess
- Oncologists tracking cancer spread
- Surgeons planning adrenalectomy
Imaging Modalities & Protocols
Which CT protocol should you use?
Follow a dedicated adrenal gland CT scan protocol: start with a noncontrast phase, then a rapid arterial phase at about 70seconds, and finally a delayed phase at 10minutes. This threestep approach lets you calculate washout percentagesa key to telling benign from malignant.
When is MRI preferable?
If the patient has a contrast allergy, wants to avoid radiation, or you need better softtissue contrast, MRI steps in. Chemicalshift sequences (in and outofphase) are especially useful for spotting intracellular lipid, a hallmark of adenomas.
Can PET/CT help?
Fluorodeoxyglucose (FDG) PET/CT shines when you suspect metastasis. High FDG uptake typically flags a malignant lesion, while benign adenomas stay relatively dark.
Technical pitfalls to watch for
Low tube voltage can artificially raise Hounsfield units (HU), and improper ROI placement may skew washout values. Keeping these variables in check is critical for reliable adrenal washout radiology.
| Modality | Resolution | Radiation | Cost | BestFit Lesion |
|---|---|---|---|---|
| CT | High | Yes | Moderate | Adenoma, Myelolipoma, Metastasis |
| MRI | Very High | No | Higher | Pheochromocytoma, Lipidpoor Adenoma |
| PET/CT | Variable | Yes | High | Metastasis, Functional Tumors |
Key Imaging Characteristics
Adrenal Adenoma (radiology)
Benign adenomas usually sit at 10HU on a noncontrast scan. If the precontrast number is higher, you can still call it benign when the absolute washout exceeds 60% or the relative washout tops 40% on the 10minute delayed image.
Adrenal Myelolipoma (radiology)
This rare, fatty tumor looks like a negative HU valueoften under30HUbecause of the macroscopic fat inside. MRI will show a signal drop on fatsuppressed sequences.
Pheochromocytoma
On MRI, pheochromocytomas light up like a lightbulb on T2weighted images. On CT they enhance strongly in the arterial phase and often stay bright on delayed scans.
Adrenal Metastasis
Metastatic lesions typically have >10HU on the noncontrast scan and washout percentages below 40%. Their borders are irregular, and they may calcify.
Cysts & Hemorrhage
Simple cysts have waterlike attenuation (02HU) and a thin wall with no enhancement. Acute hemorrhage is hyperdense initially and mellows over weeks.
| Lesion | Typical HU | Washout (%) | MRI Signal | Key Feature |
|---|---|---|---|---|
| Adenoma | 10 | Abs>60% / Rel>40% | Iso to slightly hyperintense | Intracellular lipid |
| Myelolipoma | 30to100 | N/A | Fat suppression loss | Macroscopic fat |
| Pheochromocytoma | 3050 | Low | Bright T2 lightbulb | Vascular |
| Metastasis | >10 | <40% | Variable | Irregular margins |
Using the Adrenal Washout Calculator
How do you compute absolute washout?
Plug the numbers into this simple formula:
Absolute=(PrecontrastHUDelayedHU)(PrecontrastHUPortalphaseHU)100%
For example, if the precontrast value is 25HU, the portalphase (postcontrast) reading is 70HU, and the delayed scan reads 30HU, the absolute washout works out to 57%just shy of the 60% cutoff, indicating you need more information.
When is the calculator reliable?
It gives trustworthy results when you use a consistent ROI of at least 1cm, keep the CT tube voltage at 120kVp or higher, and acquire the delayed phase exactly at 10minutes.
Can PACS automate this?
Many modern PACS packages (like GEs Advantage or Siemens Syngo) have builtin washout tools that automeasure the ROI and output percentagessaving you from manual calculations. Just make sure to doublecheck the timing settings.
What if washout is indeterminate?
When the numbers land in a gray zone, the next step is usually a chemicalshift MRI or a repeat CT with a slightly altered protocol. In some cases, a biopsy may be warranted, especially if the patient has known cancer.
Differential Diagnosis Workflow
Fast algorithm to rule out malignancy
- Measure noncontrast HU. 10HU? Likely adenoma.
- If >10HU, calculate washout. Absolute>60% or relative>40%? Benign adenoma.
- Check for macroscopic fat on CT. Negative HU? Myelolipoma.
- Review MRI chemicalshift. Loss of signal on outofphase? Lipidrich adenoma.
- Consider clinical context (known cancer, hypertension). If high risk, proceed to PET/CT or biopsy.
Visual flowchart (for graphic designers)
Start Noncontrast HU 10? Yes Benign Adenoma End
No Calculate Washout >60%/40%? Yes Benign Adenoma End
No Check Fat Negative HU? Yes Myelolipoma End
No MRI ChemicalShift Signal loss? Yes Lipidrich Adenoma End
No Clinical Risk? High PET/CT or Biopsy End
Common Pitfalls & How to Avoid Them
Tube voltage tricks
Using a low kVp (e.g., 80kVp) artificially raises HU, making a benign lesion look suspicious. Stick to 120kVp for adrenal protocols.
ROI placement errors
Including adjacent liver or kidney tissue in your region of interest can inflate washout percentages. Keep the ROI snug inside the lesion, avoiding edges.
Timing mistakes
Delayed images taken at 5minutes instead of the recommended 10minutes often underestimate washout, leading to falsepositive concerns.
Lipidpoor adenomas masquerading as cancer
These lesions sit at >10HU but still wash out well. Without a proper washout calculation, they can be mistaken for metastasis. Thats why the stresses the importance of the delayed phase.
Clinical Management Implications
When is surgery indicated?
Typical thresholds: size >4cm, growth rate >1cm per year, or functional hormone excess. Even a small lesion that secretes excess cortisol or catecholamines often warrants removal.
Endocrine workup based on imaging
If the imaging suggests an adenoma, youll still want a baseline hormonal panel (aldosterone, cortisol, catecholamines) to rule out a silent secreting tumor.
Followup schedule
Indeterminate lesions usually get a repeat CT at 6months, then annually if stable. Benign adenomas <4cm with classic imaging can be discharged after one confirming scan.
How to talk to patients
Explain the numbers in plain language: Your lesion measures 8HU, which is like the density of water, and it washes out 70% in ten minutesboth signs that its almost certainly harmless. This reassurance reduces anxiety and builds trust.
Conclusion
Adrenal imaging findings give us a powerful, numbersdriven map for sorting harmless innocent bystanders from potentially dangerous lesions. By mastering the adrenal gland CT scan protocol, using the adrenal washout calculator, and staying aware of common pitfalls, you can make confident, evidencebased decisions while sparing patients unnecessary procedures. Keep the workflow chart handy, doublecheck your ROI, and remember that every scan is a story waiting to be toldsometimes the story is a simple, benign adenoma, and sometimes its a cue to act fast.
Want a printable version of the flowchart or a quickaccess washout calculator? Grab them below and feel free to drop a comment with your own imaging adventures. Were all in this together, learning one scan at a time.
For clinicians managing endocrine causes related to adrenal findings, consider reviewing guidance on adrenal tumor growth rate to help determine appropriate surveillance intervals and thresholds for intervention.
FAQs
What HU value on a non‑contrast CT suggests a benign adrenal adenoma?
Typically ≤ 10 HU. Lesions with higher attenuation need wash‑out calculation for further assessment.
How is absolute wash‑out calculated for adrenal lesions?
Absolute = (Pre‑contrast HU – Delayed HU) ÷ (Pre‑contrast HU – Portal‑phase HU) × 100 %.
When should MRI be preferred over CT for adrenal evaluation?
MRI is favored for patients with contrast allergy, to reduce radiation exposure, or when chemical‑shift imaging is needed to detect intracellular lipid.
What imaging feature distinguishes a myelolipoma from other adrenal masses?
Myelolipomas contain macroscopic fat, appearing as negative HU (‑30 to ‑100) on CT and losing signal on fat‑suppressed MRI sequences.
Which adrenal lesions require surgical removal?
Indications include size > 4 cm, growth > 1 cm per year, or functional hormone excess (e.g., cortisol, catecholamines) regardless of size.