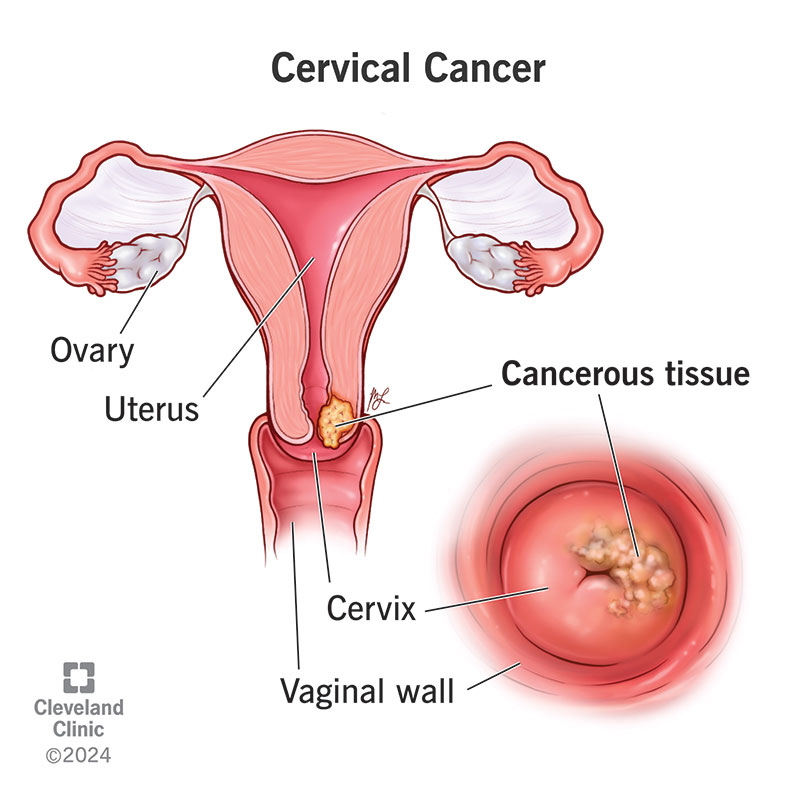
Looking for a clear, uptodate walkthrough of cervicalcancer staging on Radiopaedia? Below youll find the FIGFIGO and TNM systems, the imaging tricks radiologists rely on, and realcase screenshots that let you stage a tumor in minutes.
Why Staging Matters
Imagine trying to navigate a city without a mapyoud end up lost, right? Staging works the same way for cervical cancer. It tells doctors which neighbourhood the tumor lives in, how far it has traveled, and what routes are still open for treatment. The benefit? A treatment plan thats precisely tailored, sparing you unnecessary surgery or chemo. The risk? Overstaging can push a patient toward overly aggressive therapy, while understaging might miss hidden spread, reducing chances of cure.
Dr.EmilyHart, a gynecologic oncologist with 15years of experience, often says, Staging is the roadmap for curative versus palliative intent. That simple truth underscores why we need a reliable, imagedriven approachsomething Radiopaedia delivers with both depth and clarity.
FIGO vs TNM
The Current FIGO System (2024 Update)
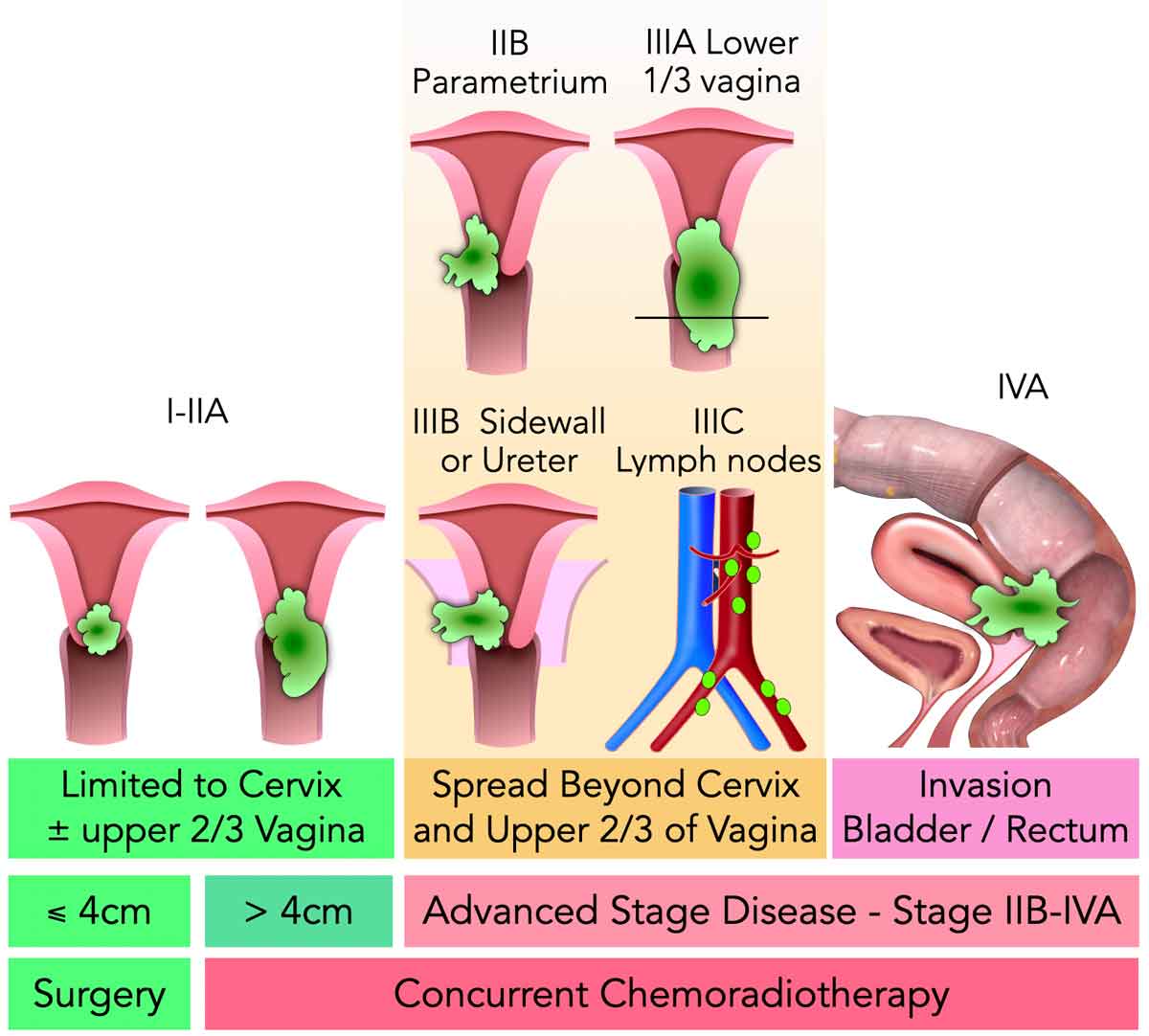
The International Federation of Gynecology and Obstetrics (FIGO) revamped its staging in 2018 and added a 2024 refinement that sharpens the role of imaging. The stages run fromI (confined to the cervix) toIV (distant spread), with subcategories like IA1, IB2, IIIC1, and so on. The big change? Nodal disease now has its own categoryIIIC1 for pelvic nodes andIIIC2 for paraaortic nodesmaking MRI and PETCT essential tools.
Comparison Table FIGO vs TNM
| Feature | FIGO (2018/2024) | TNM (8thEdition) | Typical Imaging Modality |
|---|---|---|---|
| Sizebased criteria | Yes (tumor diameter) | T (size) + N (nodes) | MRI |
| Lymphnode involvement | Added in 2018 (IIIC) | Nstage (N1N3) | MRI / PETCT |
| Clinical vs. radiologic | Clinical; now imagingaugmented | Radiologic | CT, MRI, PETCT |
| Parametrial invasion | Assessed by exam & imaging | T2b (parametrial) | MRI |
When to Use TNM Instead of FIGO
TNM shines in research trials and when surgeons need a radiologic gold standard. It breaks disease down into T (tumor), N (nodes), and M (metastasis) components, giving a granular pictureespecially useful when planning complex multimodal therapy.
Imaging Role
MRI: The GoldStandard (Radiopaedia Highlights)
According to a , MRI excels at softtissue contrast, letting us see the exact depth of stromal invasion, parametrial spread, and even tiny nodes as small as 5mm. T2weighted sagittal and axial planes are the workhorses; DET2 or diffusionweighted imaging adds extra confidence when the tumor is tucked close to the bladder or rectum.
Typical MRI Findings per FIGO Stage
- StageIA: No visible lesion on MRI, but pathology shows microinvasion.
- StageIB1/IB2: Tumor confined to the cervix, measured <20mm (IB1) or 2040mm (IB2).
- StageIIB: Clear parametrial thickening or signal change crossing the cervical stroma.
- StageIIIC1: Enlarged pelvic nodes with restricted diffusion.
- StageIVB: Distant organ involvementoften seen on PETCT rather than MRI.
CT & PETCT When They Complement MRI
CT is quick and great for assessing bone involvement or largescale abdominal spread, while PETCT lights up metabolically active nodes that might look innocuous on MRI. Together they give a full picture, especially in advanced stages where distant metastasis is a concern.
Ultrasound & Other Modalities (Brief Note)
In lowresource settings, transvaginal ultrasound can flag a bulky lesion, but it struggles with parametrial invasion. Knowing its limits helps clinicians decide when to upgrade to MRIbalancing benefits and risks responsibly.
StepbyStep Staging
StageI (IAIB)
Start with the tumors greatest dimension on T2weighted images. If its <5mm and confined, youre looking at IA1. Between 515mm, IA2. Anything larger but still within the cervix lands you in IB1 or IB2, depending on the 20mm cutoff. Radiopaedias case library offers sidebyside examplesyoull spot the difference in a flash.
ImageAnnotation Checklist
- Measure maximal craniocaudal length.
- Note any stromal disruption.
- Check for involvement of the uterine corpus.
- Document any suspicious nodes, even if subcentimeter.
StageII (IIAIIB)
Parametrial invasion is the starring feature here. Look for highsignal intensity extending beyond the cervical stroma into the parametrial fat on T2. If the vaginal fornix is involved but parametrial tissue is clear, youre at IIA. Add parametrial spread and you jump to IIB.
Sample Radiopaedia Case StageIIIC1
Radiopaedias StageIIIC1 pelvic nodal disease case (case#8) shows a 6mm node with bright diffusion restrictionexactly the kind of detail that upgrades a patient from IIB to IIIC1, altering the treatment plan from surgery alone to chemoradiation.
StageIII &IV (IIIAIVB)
When the tumor reaches the pelvic sidewall, bladder, or rectum, youre in IIIA or IIIB. The presence of nodal disease (IIIC1/IIIC2) pushes the stage higher, regardless of local size. Distant spread to lungs, liver, or bones lands a patient in IVBusually seen on PETCT.
DecisionTree Flowchart (Textual)
Start Measure tumor size Check stromal invasion Look for parametrial spread Identify nodal disease Assess distant metastasis. Follow each yes or no branch and youll land at the correct FIGO stage.
Reporting Checklist
Standard Reporting Template (Radiopaedia Style)
Consistent reports help multidisciplinary teams act quickly. A solid template includes:
- Patient identifiers and imaging protocol.
- Tumor dimensions (craniocaudal, anteroposterior, transverse).
- Depth of stromal invasion.
- Parametrial, vaginal, and bladder/rectal involvement.
- Node assessment size, location, diffusion characteristics.
- Stage assignment with confidence level.
- Recommendation for further imaging if needed.
Common Pitfalls & How to Avoid Them
- Mistaking ovarian cysts for parametrial spread Review the fat plane; cysts usually sit outside the parametrial fat.
- Underreporting small nodes Use diffusionweighted images; even a 5mm node with high signal merits mention.
- Confusing posttreatment fibrosis with residual tumor Compare pre and posttherapy scans; fibrosis usually shows lowsignal intensity on T2.
RealWorld Cases
CaseA StageIIB (Radiopaedia Case#4)
Jane, a 42yearold, presented with heavy bleeding. MRI revealed a 3cm cervical mass breaching the parametrial fat. The radiology assistant highlighted the highsignal rim on T2, and the multidisciplinary team opted for chemoradiation. Six months later, repeat MRI showed complete responseproof that accurate staging steers therapy in the right direction.
What I Learned
Even a small parametrial invasion can tip the scale toward nonsurgical management. It taught me to never underestimate the subtle hyperintense streaks on T2those are the clues that change lives.
CaseB StageIIIC1 (NodePositive)
Mark, 55, had an incidental finding on PETCT: a 6mm pelvic node with SUV>4.5. MRI confirmed restricted diffusion. The radiology assistant flagged this as IIIC1, prompting the oncologists to add concurrent chemotherapy to the radiation plan. The outcome? Mark remained diseasefree at twoyear followup.
Evidence Quote
MRI detects nodal disease in >80% of cases, notes a 2020 study in the . Marks story lines up perfectly with that data.
Staying Updated
Radiopaedia Free & Subscription Content
Radiopaedia constantly refreshes its cervicalcancerstaging page, adding new cases and peerreviewed notes. Bookmark the Cervical Cancer Staging section and sign up for the monthly newsletterknowledge that updates itself, no extra effort required.
Radiology Assistant & RSNA Journals
The Radiology Assistants Cervical Cancer MR Staging article (2023) breaks down each sequence with annotated imagesideal for quick revision before a tumor board. Meanwhile, RSNAs annual review articles compile the latest evidence on FIGO updates and imaging techniques.
Suggested Reading List
- FIGO Staging Classification for Cervical Cancer 2020 Update (doi:10.1148/rg.2020200013).
- AJR Review: MRI in Cervical Cancer Staging (doi:10.2214/AJR.23.29003).
- Radiopaedia Cases Library cervical cancer staging series.
Conclusion
Staging cervical cancer isnt just a checklist; its the compass that guides every treatment decision. With the 2018/2024 FIGO revisions, MRI has become the cornerstonemaking Radiopaedias imagerich tutorials more relevant than ever. By using a stepbystep checklist, recognizing common pitfalls, and staying tuned to trusted resources like the Radiology Assistant and RSNA journals, you can stage a tumor confidently and help ensure patients receive the right therapy at the right time.
Weve walked through the whole process togethernow its your turn. If youve encountered a tricky case or have a question about a particular imaging sign, feel free to reach out. Lets keep learning and supporting each other on this journey toward better, more accurate cancer care.
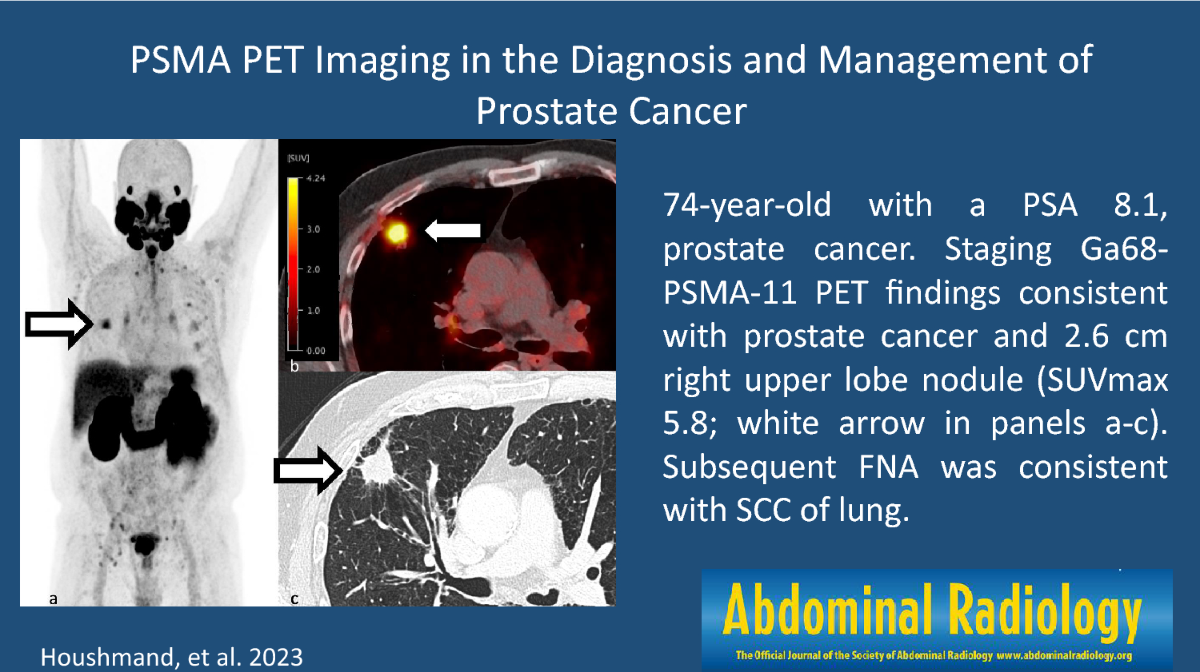
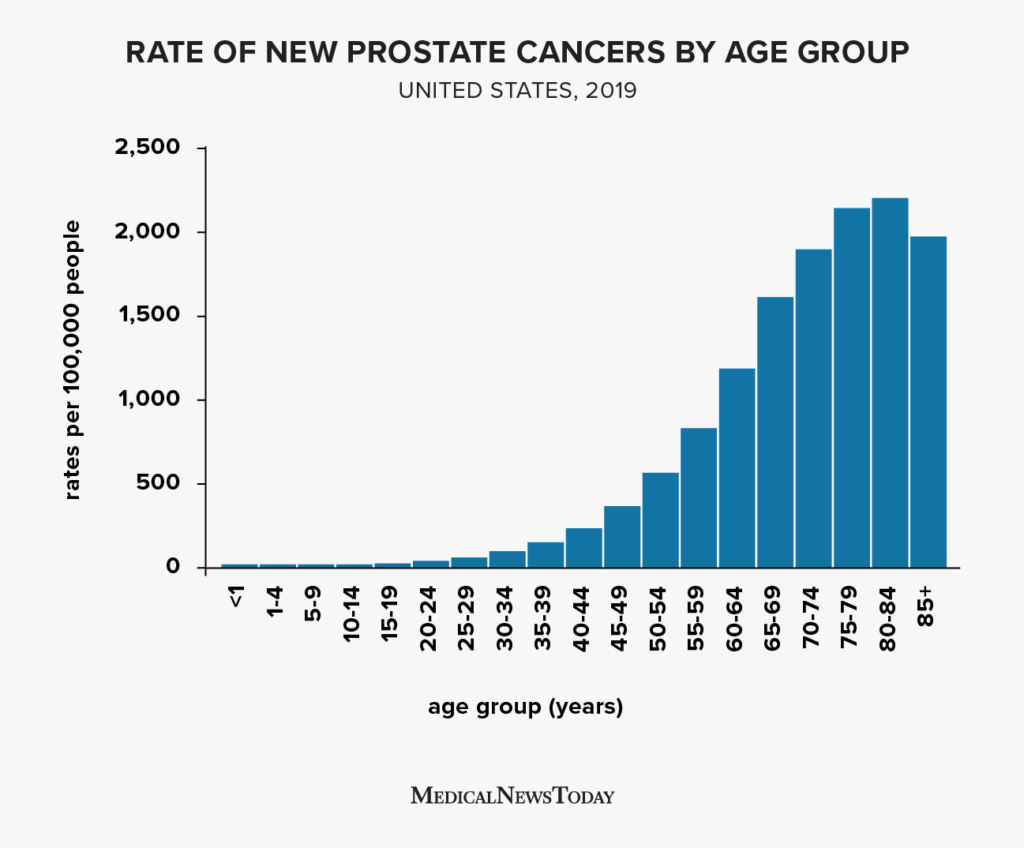
For clinicians managing treatment plans where patient prognosis and survivorship issues arise, see prostate cancer outlook for a concise example of how staging and nodal status change therapeutic intent.
FAQs
What are the main cervical cancer staging systems shown on Radiopaedia?
The primary staging systems detailed on Radiopaedia for cervical cancer are the FIGO system, updated in 2018 and refined in 2024, and the TNM system (8th edition). FIGO focuses on clinical and imaging findings, while TNM provides a detailed radiologic classification of tumor (T), lymph nodes (N), and metastasis (M).
Why is MRI considered the best imaging for cervical cancer staging?
MRI offers superior soft tissue contrast that allows precise assessment of tumor size, stromal invasion, parametrial spread, and nodal disease, making it the gold standard imaging modality for staging cervical cancer as emphasized by Radiopaedia.
What is the significance of the 2018 and 2024 FIGO updates?
The 2018 FIGO revision incorporated imaging and pathology for staging and introduced nodal status categories (IIIC1 for pelvic nodes, IIIC2 for paraaortic). The 2024 update further sharpens imaging roles, positioning MRI and PET/CT as essential tools for accurate nodal and metastatic assessment.
When should the TNM system be preferred over FIGO for staging?
The TNM classification is particularly valuable in clinical research trials and for surgical planning as it provides a granular radiologic assessment of tumor size, nodal involvement, and metastasis, complementing FIGO by offering detailed imaging-based staging.
What common pitfalls might occur during cervical cancer imaging staging?
Common pitfalls include mistaking ovarian cysts for parametrial spread, underreporting small lymph nodes without diffusion-weighted imaging, and confusing posttreatment fibrosis with residual tumor; recognition of these helps improve accuracy in Radiopaedia-based staging.