Most adrenal adenomas grow less than 3mm per year, and only about onethird actually get bigger. Knowing that growth rate helps you and your doctor decide whether to watch, test, or operate. Lets break it down together, step by step, so you feel confident about the numbers on your scan.
Understanding Growth Rate
When we talk about the adrenal adenoma rate, were really talking about how quickly the little tumor changes size over time. Its measured in millimeters per year (mm/yr). Think of it like the speedometer on a car: the slower the speed, the less urgency you have to pull over and check the engine.
What Does Growth Rate Mean?
Its simply the difference in the nodules longest dimension between two imaging studies, divided by the time elapsed. For example, a lesion thats 1.5cm today and 1.6cm after 12months has a growth rate of 0.1mm/yr.
Why Clinicians Track It
Because the rate tells us a lot about the lesions behavior. A slowgrowing or stable adenoma usually means its benign and can be safely watched. A fastergrowing nodule raises a flag: maybe its edging toward the size where surgery becomes advisable, or perhaps it signals a functional tumor that needs hormone workup.
Key Stats from Recent Research
| Study | Median Growth | Range |
|---|---|---|
| J. Clin. Endocrinol. (2022) | 0.3mm/yr | 02.8mm/yr |
| AJR (2020) | 0.5mm/yr | 3mm/yr for 90% of lesions |
| Radiopaedia Review | 0.2mm/yr | 05mm/yr (rare outliers) |
These numbers come from large cohorts of patients who had incidental adrenal nodules discovered on CT scans. The takeaway? Most lesions barely budge.
How Fast They Grow
Lets get into the nittygritty of actual growth patterns. Imagine youre watching a plant sprout; some seeds barely sprout, others shoot up quickly.
Average Growth on CT Scans
Across dozens of studies, the median growth hovers around 0.3mm/yr. Thats roughly the thickness of a single sheet of printer paper per yearpractically invisible to the naked eye.
Range of Observed Rates
While most adenomas stay under 3mm per year, a few outliers grow up to 2.8mm/yr. Its still a snails pace compared to malignant adrenal cortical carcinoma, which can expand more than 10mm/yr.
How Malignant Lesions Differ
Adrenocortical carcinoma (ACC) typically shows a rapid growth patternoften >13mm/yr. If your scan shows a nodule increasing that fast, your doctor will likely order additional imaging and labs right away. , such rapid growth is a red flag for malignancy.
Benign vs. ACC Comparison
| Feature | Benign Adenoma | ACC |
|---|---|---|
| Typical Growth | 0.20.5mm/yr | 1015mm/yr |
| Size at Diagnosis | 4cm | 5cm |
| CT Attenuation | 10HU (noncontrast) | Variable, often >20HU |
Measuring the Rate
Getting an accurate growth rate isnt magic; its science combined with a bit of meticulous recordkeeping.
CT Measurement Protocol
Radiologists use thinslice (1mm) noncontrast CT images to measure the longest diameter of the nodule. They repeat the scan after a set intervalusually 612months for new lesions, then annually if stable.
Using an Adrenal Adenoma Calculator
There are webbased tools that let you input the initial size, the followup size, and the time between scans. The calculator spits out the growth rate (mm/yr) and can even suggest a surveillance schedule.
StepbyStep Example
Imagine Janes nodule was 1.8cm on her first CT. Twelve months later, it measured 1.92cm.
- Difference = 0.12cm = 1.2mm
- Time = 12months = 1year
- Growth rate = 1.2mm/yr
Plugging those numbers into an confirms a rate of 1.2mm/yr, which is still below the 3mm/yr fast threshold but above the median.
Size & Growth Thresholds
Size mattersboth the absolute measurement and how fast its changing.
Size Criteria
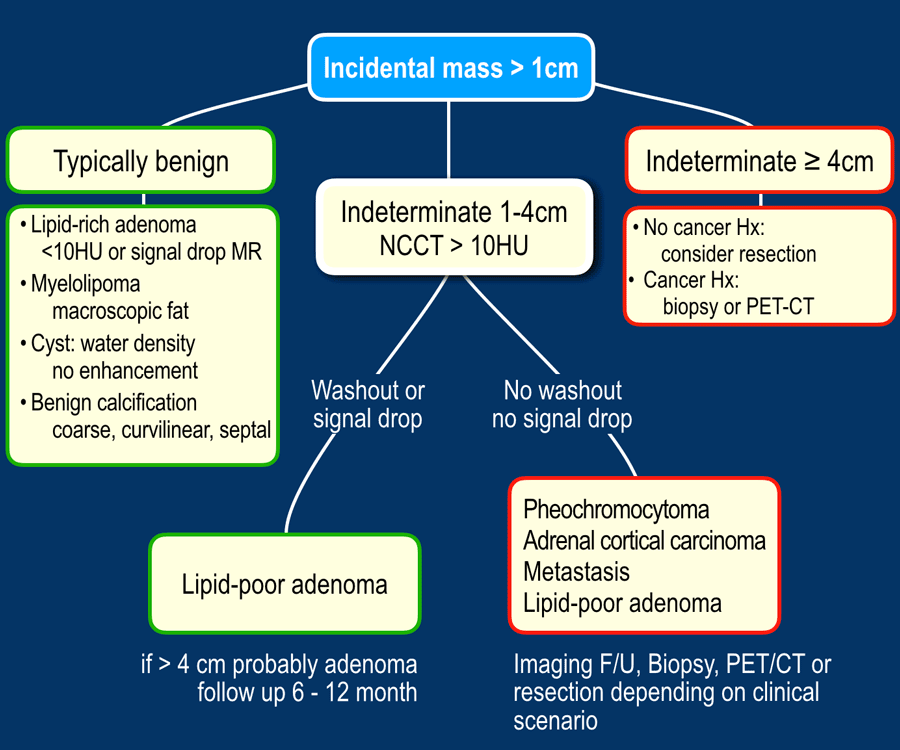
Guidelines generally consider lesions 4cm with 10HU on noncontrast CT as presumed benign. Anything larger, or with higher attenuation, warrants a closer look.
Growth Thresholds Prompting Surgery
Most experts agree that if a nodule grows >5% per year or gains more than 0.5cm in absolute size, its time to discuss surgical removalespecially if the lesion is already near the 4cm mark.
DecisionMaking Flowchart
| Step | Action |
|---|---|
| Initial detection | Noncontrast CT, measure size & HU |
| Year1 followup | Repeat CT if >1cm or borderline HU |
| Growth <0.5cm/yr | Continue surveillance every 1224months |
| Growth 0.5cm/yr or >5%/yr | Discuss adrenalectomy |
Symptoms & Workup
Most adrenal adenomas are silentthey dont make you feel anything. But some secrete hormones, turning a quiet tumor into a noisy troublemaker.
When Growth Matters Clinically
If the nodule is functional (producing excess cortisol, aldosterone, or catecholamines), even a tiny size change can be important because hormone excess can cause high blood pressure, weight gain, or anxiety.
Key Blood Tests
Doctors usually order a panel that includes:
- Serum cortisol (overnight dexamethasone suppression)
- Plasma metanephrines (for pheochromocytoma)
- Aldosteronerenin ratio (for primary aldosteronism)
Abnormal results push the workup from watchful waiting to active treatment regardless of the growth rate.
LabResult Interpretation Table
| Test | Normal | Suspicious |
|---|---|---|
| Cortisol (postdex) | Suppressed | 5g/dL Cushings risk |
| Metanephrines | Within reference | Elevated Pheochromocytoma |
| AldosteroneRenin Ratio | 20 | >30 Primary Aldosteronism |
Treatment Options
Deciding whether to intervene is like choosing between a plain coffee and a fancy latteyou weigh the benefits, costs, and personal taste.
Active Surveillance
Most patients stay on surveillance. Typical schedule: repeat CT at 612months, then annually for the first two years if unchanged. This approach preserves quality of life and avoids surgery risks.
Surgical Intervention
When the nodule breaches size or growth thresholdsor if its hormonally activelaparoscopic adrenalectomy is the gold standard. Robotic assistance is becoming more common, offering precise dissection and quicker recovery.
Risks vs. Benefits Matrix
| Aspect | Surveillance | Surgery |
|---|---|---|
| Mortality | Near zero | 0.51% (centerspecific) |
| Hormone remission | Depends on function | 95% for cortisolproducing adenoma |
| Recovery time | None | 12weeks (laparoscopic) |
| Longterm followup | Annual imaging | Usually none after complete removal |
RealWorld Cases
Stories help turn numbers into human experience. Below are two anonymized cases that illustrate the spectrum of adrenal adenoma behavior.
Case A The Slow Grower
Mark, 58, had a 1.4cm incidentaloma discovered during a CT for kidney stones. Over five years of annual scans, the lesion nudged from 1.4cm to 1.5cm a growth rate of just 0.2mm/yr. Hormone panels were flat. The decision: continue surveillance. Mark never needed surgery and lives anxietyfree.
Case B The Fast Grower
Sara, 45, presented with hypertension and a 2.2cm adrenal nodule. Within 18months, it swelled to 2.9cm a rate of ~4mm/yr, well above the fast cutoff. Blood tests revealed elevated metanephrines, confirming a pheochromocytoma. She underwent laparoscopic adrenalectomy, recovered in 10 days, and her blood pressure normalized.
Takeaway Lessons
- Even modest growth can be a signal if hormone tests are abnormal.
- Stable lesions over many years rarely need surgery.
- Personalized followup (size, rate, labs, patient preference) beats a onesizefitsall approach.
Key Takeaways
Lets wrap up what weve learned, in plain language:
- Most adenomas grow slowly. The median adrenal adenoma rate is about 0.3mm/yrso slow you might not notice.
- The growth rate guides decisionmaking. A rate under 0.5mm/yr usually means watchful waiting; over 0.5mm/yr or >5% per year steers doctors toward surgery.
- Combine imaging with labs. Hormone tests (cortisol, metanephrines, aldosterone) can turn a quiet nodule into an urgent matter, regardless of size.
- Size matters, but so does change. Lesions 4cm with low CT attenuation are often benign; rapid enlargement pushes the threshold lower.
- Personal stories matter. Realworld cases show that both slow growers and fast growers exist, and each patients journey is unique.
If youve found an adrenal nodule in your scans, dont panic. Talk with your endocrinologist or radiologist about the specific growth rate, hormone panel, and your own comfort level. And if you want a quick way to calculate that rate, grab a free its as easy as plugging in two numbers.
Whats your experience with adrenal imaging? Have you ever felt the stress of waiting for a followup scan? Share your story in the comments; together we can turn anxiety into knowledge.
For more on how tumors behave over time and what to expect during followup, this primer pairs well with discussions on adrenal tumor growth rate to give you practical measurement examples and surveillance timelines.
FAQs
What is considered a normal adrenal adenoma growth rate?
Most adrenal adenomas grow ≤ 0.5 mm per year, with a median rate around 0.3 mm/yr. This slow pace usually signals a benign lesion that can be safely observed.
How often should I have imaging follow‑up for an adrenal incidentaloma?
Initial follow‑up is typically at 6–12 months. If the nodule is stable, annual scans for the next 1–2 years are common, then every 2–3 years if no changes occur.
When does an adrenal adenoma require surgery?
Surgery is considered when the lesion grows > 0.5 cm/yr or > 5 % per year, reaches ≥ 4 cm, shows suspicious CT features, or is hormonally active.
Can a small adrenal adenoma cause hormone problems?
Yes. Even a tiny adenoma can secrete excess cortisol, aldosterone, or catecholamines, leading to Cushing’s syndrome, primary aldosteronism, or pheochromocytoma, regardless of size.
How is the adrenal adenoma growth rate calculated?
Subtract the initial longest diameter (in mm) from the follow‑up diameter, then divide by the number of years between scans. The result is the growth rate in mm/yr.