Hey there, I know that hearing androgen deprivation therapy (or ADT for short) can feel like stepping into a maze of acronyms and medical jargon. Lets cut through the noise together. In a nutshell, ADT is a group of medicines that lower testosterone or block its action, because prostate cancer cells love that hormone. Below youll find the full roster of drugs, why doctors pick one over another, and what you can expect on the road ahead.
Quick Overview
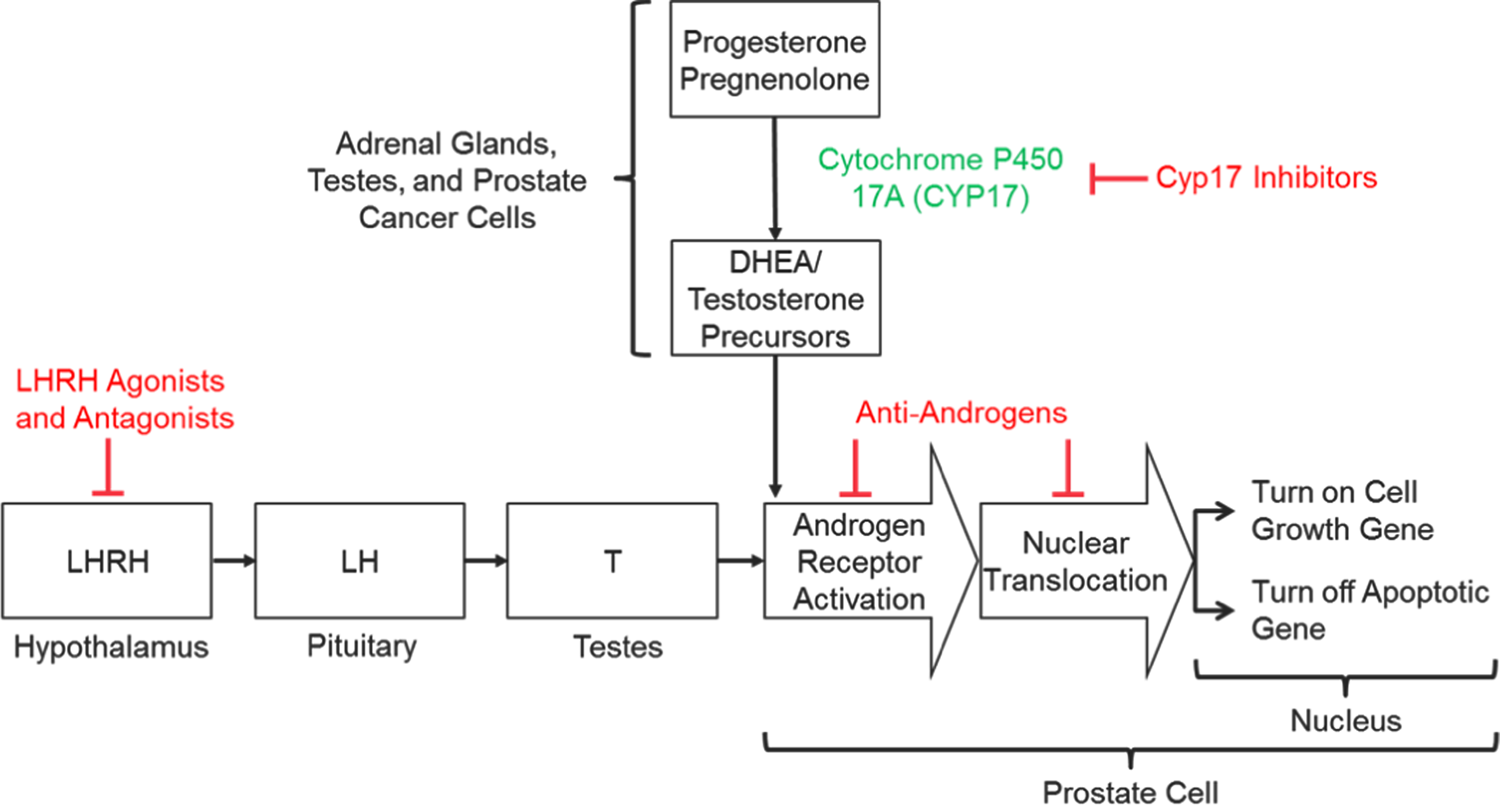
Think of ADT as a twostep plan: first, turn down the bodys testosterone production, then block any remaining testosterone from humming its way into cancer cells. The drugs fall into three broad familiesLHRH agonists, LHRH antagonists, and antiandrogens (plus a few synthesis blockers). Each family has its own rhythm, sideeffect vibe, and convenience level.
Core Drug Classes
| Class | Generic(s) | Brand(s) | Formulation | Typical Frequency |
|---|---|---|---|---|
| LHRH Agonists | leuprolide, goserelin, triptorelin, histrelin, buserelin | Lupron, Zoladex, Pamorelin | Injectable depot (S.C. or I.M.) | Every 1, 3, or 6 months |
| LHRH Antagonists | degarelix, relugolix | Firmagon, Orgovyx | Subcutaneous injection (degarelix) / oral (relugolix) | Every 1 month (degarelix) or daily (relugolix) |
| Androgen Synthesis Inhibitors | abiraterone, ketoconazole | Zytiga, Noxafil | Oral tablets | Daily |
| FirstGen Antiandrogens | bicalutamide, flutamide, nilutamide | Casodex, Eulexin, Nilandron | Oral tablets | Daily |
| NextGen Antiandrogens | enzalutamide, apalutamide, darolutamide | Xtandi, Erleada, Nubeqa | Oral tablets | Daily |
All of these drugs are approved by the FDA for various stages of prostate cancer. The exact combosay, leuprolide plus bicalutamidedepends on your cancers aggressiveness, your health profile, and sometimes just personal preference (injection vs. pill, for example).
Detailed Look
LHRH Agonists The Classic Choice
These guys mimic the bodys own luteinizinghormonereleasing hormone, causing an initial testosterone surge before the pituitary shuts down. That surge can be a bit of a headache, so doctors often give a shortacting antiandrogen at the start to blunt it.
- Typical sideeffects: hot flashes, mild injectionsite pain, occasional mood swings.
- Convenient dosing: many men love the 3month depot (leuprolide) because its just a quarterly office visit.
Leuprolide Dosing Options
| Package | Frequency | Amount per Injection |
|---|---|---|
| 1Month | Every month | 7.5 mg |
| 3Month | Every 3 months | 22.5 mg |
| 6Month | Every 6 months | 45 mg |
LHRH Antagonists No Surge, Faster Action
If youre not a fan of that initial testosterone spike, antagonists like degarelix or the oral relugolix skip it entirely. They bind directly to the receptors in the pituitary and shut testosterone production straight away.
- Pros: immediate testosterone suppression, no need for a flare medication.
- Cons: degarelix can cause injectionsite redness; relugolix requires daily pills and a bit more stomachfriendly timing.
Agonist vs. Antagonist Quick Comparison
| Aspect | Agonist | Antagonist |
|---|---|---|
| Onset | Weeks (flare first) | Days (no flare) |
| Typical Dosing | Monthly, 3monthly, 6monthly | Monthly injection or daily oral |
| Common Sideeffects | Hot flashes, mild pain | Injectionsite redness, GI upset (relugolix) |
| Cost (US) | Varies, often covered | Higher for oral relugolix |
FirstGeneration Antiandrogens The Blockers
These pillsbicalutamide, flutamide, nilutamidedont lower testosterone; they simply block the hormone from binding to cancer cells. Theyre often added to an LHRH drug to create a combined ADT regimen.
- Why add them? They help prevent the early flare from agonists and give a small extra push against tumor growth.
- Sideeffects: mild liverenzyme changes, occasional visual disturbances (nilutamide).
Johns Story (RealWorld Example)
John, a 68yearold from Texas, started on a 3monthly leuprolide shot after his doctor spotted a rising PSA. He felt a brief heat wave (the flare) and his urologist added bicalutamide. It felt like we were covering all bases, John told me. Six months later, his PSA dropped and he felt steadier.
NextGeneration Antiandrogens Power Players
Enzalutamide, apalutamide, and darolutamide are the newer, more potent blockers. Theyre especially useful when the cancer becomes resistant to standard ADT (socalled castrationresistant prostate cancer).
- Key benefits: stronger receptor blockade, works even when testosterone is low.
- Watch out for: fatigue, hypertension, and in rare cases, seizures (especially with enzalutamide).
SideEffect Spotlight
Patients on enzalutamide often report a brain fog. A practical tip from a Mayo Clinic article suggests scheduling dosetime when youre most alert (e.g., morning) and keeping a simple daily routine.
Androgen Synthesis Inhibitors Cutting the Supply at the Source
Abiraterone (Zytiga) blocks an enzyme needed for testosterone production in the adrenal glands and prostate. Because it also raises mineralocorticoid levels, doctors pair it with lowdose prednisone to keep blood pressure and potassium in check.
- Take with food: Abiraterone absorption jumps dramatically when taken with a fullfat meal. Set a reminder to have it with breakfast or lunch.
- Sideeffects: fluid retention, high blood pressure, liverenzyme changes.
Choosing Your Regimen
Deciding which drugor comboto use isnt a onesizefitsall answer. Here are the main ingredients that go into the decision:
- Cancer stage: Advanced or metastatic disease usually means continuous ADT, often combined with a nextgen antiandrogen.
- Other health conditions: Diabetes, heart disease, or osteoporosis can sway the choice toward agents with milder metabolic impact.
- Lifestyle preferences: Some men hate needles and prefer oral pills; others love the convenience of a quarterly shot.
- Cost & insurance: Newer drugs can be pricier. Checking with your insurer early can avoid surprise bills.
Imagine a simple flowchart: Is your cancer localized? No? Continuous ADT + consider nextgen antiandrogen. Yes? Discuss intermittent ADT or watchful waiting.
For those wrestling with the idea of refusing hormone therapy, know youre not alone. A recent study in notes that men who decline ADT should be closely monitored, and alternative options like targeted radiation may become part of the plan.
Managing ADT Side Effects
Side effects can feel like an unwanted guest that never leaves the party. Below is an ataglance guide to the most common issues and practical ways to keep them in check.
| SideEffect | Typical Drugs | Management Tips |
|---|---|---|
| Hot flashes | All ADT agents | Layered clothing, cooling pillows, consider lowdose antidepressants (per physician). |
| Loss of libido | Any ADT | Open communication with partner, counseling, possible use of PDE5 inhibitors. |
| Bone density loss | LHRH agonists/antagonists | Calcium+vitaminD, weightbearing exercise, bisphosphonates if needed. |
| Fatigue | Nextgen antiandrogens | Regular light activity, sleep hygiene, discuss dose timing. |
| Elevated blood pressure | Abiraterone | Monitor BP, lowdose prednisone helps, discuss antihypertensives. |
Dont forget mental health. Hormone changes can linger in the brain, leading to mood swings or depressive feelings. A quick chat with a therapist or a support group often makes a world of difference.
How Long Can a Man Stay on Hormone Therapy?
Theres no single oneyear rule. Duration really hinges on disease status and how well you tolerate the meds. In metastatic settings, studies show that staying on ADT for at least 23years improves survival. For localized disease, some doctors use an intermittent strategysix months on, six months offto give the body a breather and reduce sideeffect burden.
One patient I spoke with, Mark, told me: I was on continuous ADT for three years, then we tried a break. My PSA stayed low for another year, and I felt like I got my life back. Talk with your oncologist about whether an intermittent schedule could work for you.
Life After Androgen Deprivation Therapy
When the treatment window closes, testosterone gradually climbs back up. Most men notice a return of energy within a few weeks to months, but the PSA needs close monitoring to catch any early signs of recurrence.
- Followup schedule: PSA every 36months for the first two years, then annually.
- Bone health: Continue calcium, vitaminD, and weightbearing exercises even after ADT ends.
- Cardiovascular care: Keep blood pressure, cholesterol, and glucose under controlADT can leave a lingering impact.
Think of postADT life as a new chapter, not a sudden stop. Many survivors describe a second wind, where they finally feel able to travel, garden, or enjoy hobbies theyd put on hold. If you have concerns about longterm outcomes after prostate treatments, resources on prostate cancer outlook can help clarify expectations and follow-up plans.
Key Takeaways
- ADT medicines fall into three main families: LHRH agonists, LHRH antagonists, and antiandrogens (plus synthesis inhibitors).
- Choosing the right drug depends on cancer stage, health background, lifestyle, and cost.
- Sideeffects are real but manageablestay proactive with diet, exercise, and regular doctor visits.
- Treatment length varies; continuous therapy is typical for advanced disease, while intermittent schedules may suit localized cases.
- After ADT, maintain bone and heart health, and keep up with PSA monitoring to stay ahead of any changes.
If youve made it this far, youre already armed with the knowledge to ask the right questions at your next appointment. Remember, youre not alone on this journeytalk to your care team, lean on support groups, and keep the conversation open with family and friends. Got a story or a question? Share it in the comments below; were all in this together.
FAQs
Which drug class is considered the “classic” choice for ADT?
LHRH agonists such as leuprolide, goserelin and triptorelin are the traditional first‑line agents that suppress testosterone production.
What is the main advantage of LHRH antagonists over agonists?
Antagonists like degarelix and relugolix shut down testosterone production immediately without the initial testosterone surge (“flare”) seen with agonists.
When are next‑generation anti‑androgens used?
Enzalutamide, apalutamide and darolutamide are typically added for castration‑resistant prostate cancer or when stronger androgen blockade is needed.
How should abiraterone be taken to maximize absorption?
Abiraterone should be taken with a full‑fat meal (breakfast or lunch) and paired with low‑dose prednisone to control mineralocorticoid effects.
Can hormone therapy be given intermittently?
Yes, in selected men with localized disease an intermittent schedule (e.g., six months on, six months off) can reduce side‑effects while maintaining cancer control.