Quick Answer
When leukemia cells are found in the cerebrospinal fluid (CSF), it means the disease has spread from the bonemarrow into the central nervous system (CNS). This CNS involvement signals a higher disease burden, a greater chance of relapse, and usually calls for more intensive, CNSdirected therapy.
Why It Matters
The brain and spinal cord are protected by a tough barrier that many chemotherapy drugs cant cross. When leukemia breaches that barrier, it creates a sanctuary where cancer cells can hide and evade standard treatment. As a result, doctors need to add special medicines that reach the CSF, and the overall outlook can shift.
What Is Cerebrospinal Fluid?
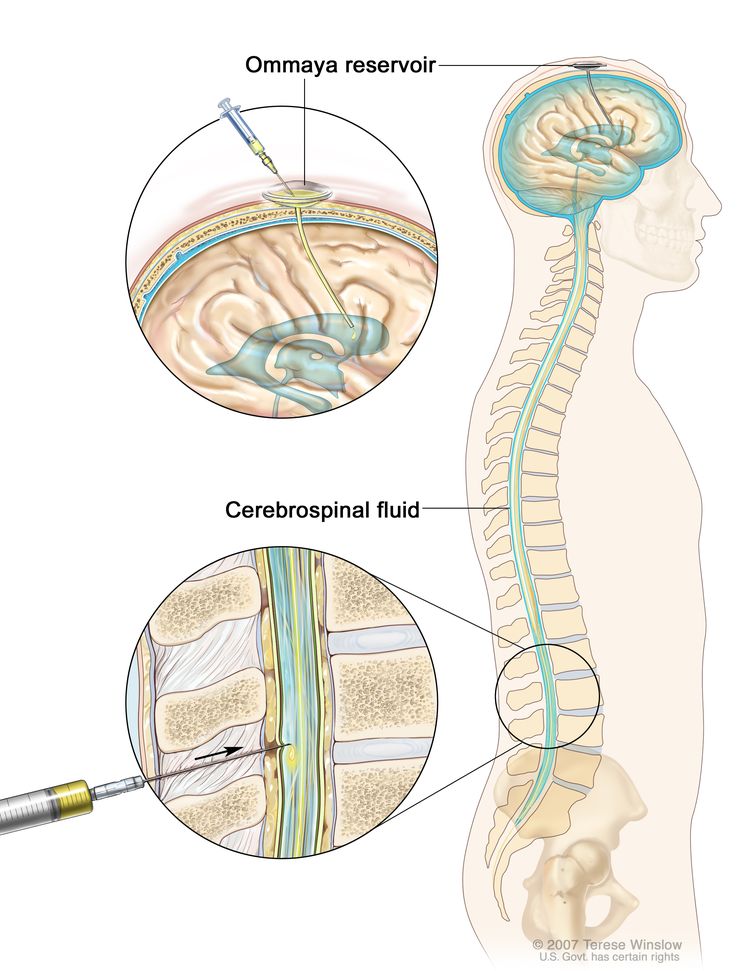
CSF is a clear liquid that cushions the brain and spinal cord, circulating through a network of ventricles and the subarachnoid space. Its the medium that carries nutrients, removes waste, and keeps our nervous system buoyant.
How Do Leukemia Cells Get In?
Leukemia can infiltrate the meninges (the membranes covering the brain and spine) or slip through tiny gaps in the bloodbrain barrier. Once there, the cells can multiply in the fluid, turning it into a hiding spot that standard systemic chemotherapy struggles to reach.
QuickFact Box
| Pathway | Typical Leukemia Types | Frequency in Kids | Frequency in Adults |
|---|---|---|---|
| Direct meningeal invasion | ALL, AML | 4% | 12% |
| Hematogenous spread | ALL, AML |
Signs & Symptoms
Because the spinal fluid is close to the brain and nerves, you may notice neurological clues. But remember, symptoms can be subtle, especially in children.
Common CNSRelated Signals
- Persistent headaches or pressure behind the eyes
- Neck stiffness or pain
- Nausea, vomiting (especially in the morning)
- Blurred vision or double vision
- Confusion, memory lapses, or sudden mood changes
- In kids, irritability, difficulty concentrating at school, or unexplained clumsiness
Children vs. Adults
Kids often cant articulate a headache, so look for behavioral changeslike being more fussy or losing interest in favorite activities. Adults may describe the headache as a pressure that doesnt go away with overthecounter meds.
RealWorld Example
Emma, a 7yearold with acute lymphoblastic leukemia (ALL), started complaining of stomach hurts and seemed unusually sleepy. A lumbar puncture revealed blasts in her CSF. The early discovery meant she could begin intrathecal therapy right away, which helped keep her disease under control.
How Its Diagnosed
The goldstandard test is a lumbar puncture, also called a spinal tap. Its a quick office procedure that lets doctors collect a small amount of CSF for analysis.
Lumbar Puncture & CSF Analysis
During the tap, a thin needle is inserted between two lower back vertebrae. The fluid is examined under a microscope for leukemia blasts, and labs measure whitecell count, protein, and glucose. According to , the presence of even a few blasts can change the entire treatment plan.
Imaging & Ancillary Tests
Doctors may also order an MRI of the brain and spine to look for any lesions or meningeal thickening. Flow cytometry and cytogenetic studies on the CSF help identify the exact leukemia subtype, which is crucial for tailoring therapy.
Patient Checklist
- Fast for 68hours before the tap (unless instructed otherwise).
- Ask about anesthesia options if youre nervous about the needle.
- Stay hydrated after the procedure to help replace lost fluid.
- Watch for headache or fever in the 24hours after; report any changes.
Prognosis & Survival
Finding leukemia in the CSF does lower survival numbers, but its not a death sentence. Modern treatments have dramatically improved outcomes, especially for children.
Overall Outlook
Studies show that patients with CNSpositive disease have a 1015% lower fiveyear survival rate compared with those whose disease stays in the marrow. The exact drop depends on the leukemia type and the patients age.
Survival Numbers by Type
| Leukemia Type | 5Year Survival (No CNS) | 5Year Survival (CNSPositive) |
|---|---|---|
| AML (adults) | 30% | 1520% |
| ALL (children) | 85% | 70% |
What Influences Prognosis?
- Specific genetic mutations (some cytogenetic profiles are more aggressive).
- Number of blasts found in the CSF.
- How quickly CNSdirected therapy is started.
- Patients age and overall health.
- Whether the leukemia is a first diagnosis or a relapse.
Treatment Options
Theres no onesizefitsall answer, but most treatment plans combine several strategies to chase leukemia out of that sanctuary.
Intrathecal Chemotherapy
This is the cornerstone. A tiny dose of chemotherapyusually methotrexate, cytarabine, or a steroidis injected directly into the CSF during a lumbar puncture. The drugs circulate throughout the CNS, knocking out the hidden cells.
HighDose Systemic Chemotherapy
Some drugs, like highdose methotrexate, can cross the bloodbrain barrier when given in large amounts. These regimens are often scheduled alongside intrathecal treatment to attack leukemia from both sides.
Targeted & Immunotherapy
Newer agents, such as tyrosinekinase inhibitors (TKIs) that penetrate the CNS, and CART cell therapy, are showing promise, especially for relapsed disease. A 2023 study in Blood reported that CNSactive TKIs improved remission rates in adult AML patients with spinalfluid involvement.
Radiation Therapy
When the disease is particularly aggressive or unresponsive, doctors may recommend cranial or craniospinal irradiation. Radiation can eradicate residual leukemia cells but carries a risk of longterm cognitive effects, especially in children.
Treatment Algorithm (Visual Flow)
- Diagnose CNS involvement via lumbar puncture.
- Start intrathecal chemotherapy (often methotrexate + cytarabine).
- Initiate highdose systemic chemotherapy that penetrates the CNS.
- Assess response; add targeted agents if indicated.
- Consider radiation for refractory cases.
- Consolidate with stemcell transplant when eligible.
Special Considerations for Kids
Pediatric protocols prioritize minimizing neurotoxicity. Doses are carefully calculated, and many centers use prophylactic intrathecal therapy early, even before any CSF blasts appear, to keep the CNS clear.
Common Questions
Below are short, snippetready answers to the questions youre probably Googling right now.
What does it mean when leukemia is in the spinal fluid?
It means leukemic cells have entered the cerebrospinal fluid, indicating central nervous system involvement and a need for CNSdirected treatment.
Leukemia in spinal fluid survival rate?
Overall fiveyear survival drops about 1015% compared with patients without CNS disease; exact numbers vary by leukemia type and age.
Leukemia in spinal fluid symptoms?
Headaches, neck stiffness, nausea, vision changes, and in children, irritability or schoolperformance decline.
Leukemia in spinal fluid treatment?
Intrathecal chemotherapy is standard, often combined with highdose systemic chemo, targeted agents, or radiation if needed.
Leukemia in spinal fluid child?
About 4% of pediatric ALL cases develop CNS involvement; treatment usually includes prophylactic intrathecal methotrexate.
What happens when leukemia spreads to the brain?
Neurological signs appear, and doctors add CNSpenetrating drugs and possibly radiation to protect brain function.
AML in spinal fluid prognosis?
Adult AML with CSF involvement typically has a 5year overall survival of 1520% under modern regimens.
What happens when leukemia spreads to the spine?
Symptoms may include back pain, leg weakness, or sensory changes, and treatment mirrors that for CSF involvementintrathecal chemo plus systemic therapy.
Balancing Benefits & Risks
Every aggressive therapy brings its own set of tradeoffs. Understanding both sides helps you make informed choices.
Benefits of Early Detection
Spotting CNS disease early lets doctors start intrathecal therapy before cancer takes hold, which improves remission rates and reduces the chance of neurologic complications.
Risks of CNSDirected Therapy
Possible sideeffects include:
- Temporary headache or chemical meningitis after a lumbar puncture.
- Infection risk from the spinal tap.
- Neurotoxicityespecially with highdose methotrexate or radiation, which can affect memory or learning.
Patient Story Sidebar
Mark, a 45yearold with AML, recalls the moment his doctor explained the need for intrathecal chemotherapy. I was terrified of another needle in my spine, but the team walked me through every step. Knowing the treatment could actually reach the hidden cells gave me hope, even when the odds seemed low. His experience underscores that the emotional cost of treatment is real, but the potential for cure can outweigh the fear.
Talking to Your Care Team
Clear communication is a twoway street. Here are a few questions you might want to bring to your next appointment.
Key Questions for Your Oncologist
- What CNSdirected regimen do you recommend and why?
- How will we monitor the CSF after each intrathecal dose?
- What are the short and longterm sideeffects I should watch for?
- Are there clinical trials for newer CNSpenetrating agents that I might be eligible for?
Support Resources
National organizations like the offer counseling, financial aid, and patienttopatient networks. Pediatric families often find comfort in local support groups that focus on coping with CNS disease.
Resources & References
All information in this article is drawn from reputable, peerreviewed sources, including recent reviews from MedicalNewsToday and the Cleveland Clinic. For the most current guidelines, always consult your hematologistoncologist.
Conclusion
Discovering that leukemia has entered the spinal fluid can feel like stepping into an unexpected shadow, but it also opens the door to targeted therapies that specifically chase cancer out of the brain and spine. By understanding the symptoms, getting a prompt diagnosis, and partnering with a knowledgeable care team, you can turn that shadow into a manageable part of the treatment journey. If you or a loved one are facing this news, reach out to your doctor today, explore reputable support networks, and rememberknowledge and timely action are powerful allies in this fight.
For patients concerned about pregnancy and leukemia treatment options, see AML pregnancy treatment for guidance on balancing maternal and fetal safety during therapy.
FAQs
What does it mean when leukemia is in the spinal fluid?
It indicates that leukemia cells have spread to the cerebrospinal fluid, showing involvement of the central nervous system and necessitating CNS-focused treatment.
What are common symptoms when leukemia spreads to spinal fluid?
Symptoms can include headaches, neck stiffness, nausea, vision changes, confusion, and in children, irritability or difficulty concentrating.
How is leukemia in the spinal fluid diagnosed?
Diagnosis is confirmed through a lumbar puncture (spinal tap) to analyze cerebrospinal fluid for leukemia cells, often supplemented by MRI and specialized lab tests.
What treatments are used for leukemia in the spinal fluid?
Treatment typically includes intrathecal chemotherapy injected directly into the cerebrospinal fluid, high-dose systemic chemotherapy, and sometimes radiation or targeted therapies.
How does leukemia in the spinal fluid affect prognosis?
Leukemia in the spinal fluid generally lowers 5-year survival rates by about 10–15%, requiring more aggressive therapy but is not a death sentence, especially with modern treatments.