Ever wonder why some asthma attacks feel like they leave a lasting scar on your lungs? The short answer is airway remodelling a structural stiffening of the bronchial walls that creeps in when inflammation sticks around for too long. It's not just a fancy medical term; it's the reason why a few people with asthma end up breathing a little harder even when they're on their usual inhalers.
In this friendly deep-dive, I'll walk you through what's happening inside those airways, why it matters, and what you (or someone you love) can actually do about it. Grab a cup of tea, settle in, and let's untangle the science together.
Understanding the Basics
What is airway remodelling in asthma?
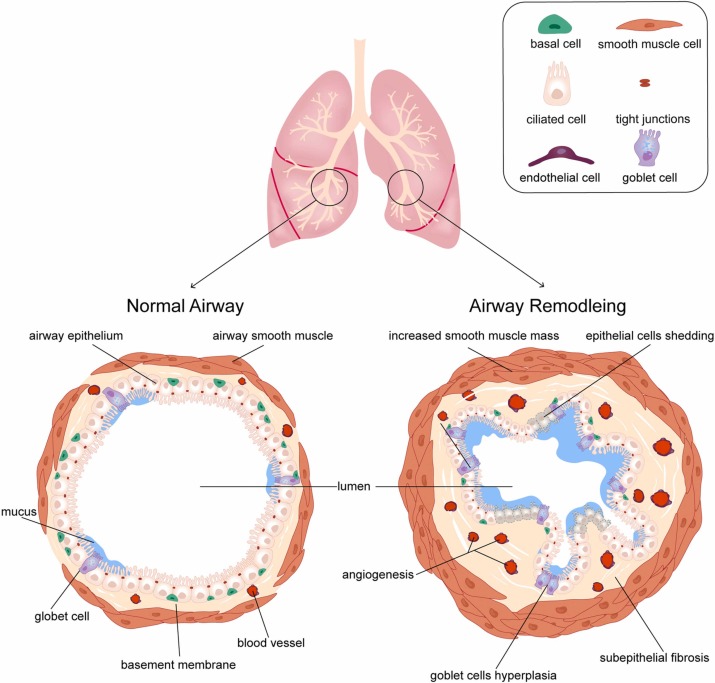
Think of your airway walls like a garden fence. In a healthy garden, the fence is flexible enough to let wind breeze through, but sturdy enough to keep the animals out. In asthma, chronic inflammation turns that fence into a rigid, overgrown wall. The remodelling part refers to three main changes:
- Thickened basement membrane a layer under the lining that gets deposited with extra collagen.
- Smooth-muscle hypertrophy the muscle around the airway gets bulkier, squeezing the airway tighter.
- Angiogenesis and fibrosis new tiny blood vessels sprout and scar tissue forms, further stiffening the passage.
All of this makes the airway less able to relax, which is why you might notice a lingering cough or a slower recovery after an asthma flare.
Why does it matter? Symptoms and life-expectancy impact
If you've ever measured your peak flow and saw numbers that just wouldn't budge, that's a hint of remodelling. Typical airway remodeling symptoms include:
- Persistent wheeze that doesn't fully disappear with rescue inhaler.
- Reduced FEV (forced expiratory volume) that stays low even after a bronchodilator test.
- Increased breathlessness during everyday activities.
Recent cohort studies show that extensive remodelling can shave a few years off airway remodeling life expectancy because the lungs lose their flexible reserve. It's not a death sentence, but it's a sign to act sooner rather than later.
Main Root Causes
Chronic inflammatory cascade the core driver
The biggest culprit is relentless inflammation. When the immune system repeatedly releases cytokines like IL4, IL5, IL13, and especially TGF, they tell the airway cells to start repairing but the repair is overzealous. Think of it as a handyman who keeps adding extra layers of paint every time you point out a scratch; eventually the walls become painfully thick.
According to the , these cytokines not only attract eosinophils (the asthma-loving white blood cells) but also trigger fibroblasts to lay down collagen, the main building block of scar tissue.
Environmental & lifestyle triggers
It's never just the cells acting alone. Dust, strong chemicals, and tobacco smoke act like irritants that keep the inflammatory alarm ringing. Even a nasty cold can give the airway lining a second hit, pushing it further toward remodeling. A 2022 PubMed review highlighted that repeated viral infections in childhood are a strong predictor of later airway stiffening. For people with overlapping conditions, considerations like cystic fibrosis safety can also influence infection risk and long-term airway health.
Genetic & epigenetic contributions
Some of us inherit a blueprint that makes our airway epithelium a bit more prone to over-repair. Genes such as ORMDL3 and FLG have been linked to exaggerated epithelial responses. Moreover, early-life exposures (like prenatal smoke or high-allergen homes) can leave epigenetic marks that keep the remodeling machinery turned on well into adulthood.
Real-world story
Meet Maya, a 28-year-old graphic designer with severe eosinophilic asthma. She was on high-dose inhaled corticosteroids (ICS) for years, yet her FEV kept slipping. A high-resolution CT scan finally showed thickened airway walls. After adding an antiIL5 biologic, her lung function stabilized and the rate of decline slowed dramatically. Maya's story reminds us that catching the process early can change the trajectory.
Is It Reversible?
Current consensus
The short answer: partially. If you intervene while the airway wall is still mostly swollen and inflamed, you can roll back some of the changes. Once fibrosis sets in that dense, scar-like tissue the remodeling becomes largely permanent.
Therapeutic windows & early intervention
Early, consistent use of high-dose ICS remains the cornerstone. A 2021 ScienceDirect study demonstrated that patients who began regular controller therapy within two years of diagnosis had up to 30% less wall thickening on follow-up scans.
Biologics targeting IL5, IL4R, or even the newer TSLP pathway have shown promise in slowing structural changes. While they aren't a magic eraser, they act like a dam, limiting the flow of inflammatory mediators that fuel remodeling.
Practical checklist for patients & clinicians
| Step | What to Do | Why It Helps |
|---|---|---|
| 1 | Confirm diagnosis with spirometry + HRCT if high risk | Identify remodeling early |
| 2 | Optimize controller therapy (ICS+LABA) | Reduce chronic inflammation |
| 3 | Consider add-on biologics for eosinophilic phenotype | Target specific cytokine pathways |
| 4 | Monitor markers (FeNO, exacerbation frequency, CT) | Track progress and adjust treatment |
Asthma vs. COPD
Common pathways
Both asthma and chronic obstructive pulmonary disease (COPD) involve airway inflammation that can lead to structural changes. TGF, for instance, drives fibrosis in both conditions. A recent review in Dove Medical Press notes that overlapping mechanisms mean some patients exhibit features of both diseases, often called asthmaCOPD overlap syndrome.
Distinct features
In asthma, the trigger is usually allergic or eosinophilic inflammation, and the airway wall thickening is often reversible early on. COPD, on the other hand, is heavily linked to long-term smoking and results in not just airway wall changes but also loss of alveolar tissue (emphysema).
Quick comparison
| Feature | Asthma-Related Remodelling | COPD-Related Remodelling |
|---|---|---|
| Primary trigger | Allergens, eosinophils | Smoking, chronic irritants |
| Typical pattern | Wall thickening, smooth-muscle hypertrophy | Airway loss, emphysema |
| Reversibility | Possible with early treatment | Generally irreversible |
Prevention & Management
Lifestyle modifications
Simple changes can make a big difference:
- No smoking even occasional exposure can tip the balance toward remodeling.
- Allergen control use HEPA filters, wash bedding weekly, and keep pets out of bedrooms if you're allergic.
- Indoor air quality humidifiers (kept clean) and regular ventilation reduce irritant buildup.
Pharmacologic approaches
Besides the backbone of inhaled corticosteroids, here's what the latest guidelines suggest:
- Biologics antiIL5 (e.g., mepolizumab), antiIL4R (dupilumab), and emerging antiTSLP agents have shown capacity to dampen the remodeling cascade.
- Long-acting muscarinic antagonists (LAMA) they relax airway smooth muscle and may have modest anti-remodeling effects.
- Combination inhalers (ICS+LABA) ensure you're using the correct technique; a bad inhaler technique can waste 50% of the dose.
Monitoring & follow-up
Consistency is key. Schedule spirometry every 612 months, and if your doctor suspects rapid progression, a low-dose high-resolution CT can give a visual map of wall thickness. Keep a simple symptom diary noting peak flow numbers, rescue inhaler use, and any triggers and bring it to each appointment. It's your personal data goldmine.
Patient-empowerment toolkit (downloadable)
Imagine having a one-page cheat sheet that you can print and keep by the bedside. It could include:
- Daily peak flow tracking table.
- Ask your doctor checklist (e.g., Should we consider a CT scan?).
- Quick tips for allergen avoidance.
Feel free to email me, and I'll send you a clean PDF version you can customize.
Future Directions The New Era of Airway Epithelium Research
Emerging targets
Scientists are now looking beyond the usual suspects. Interleukin25 (IL25) has been identified as a driver of the angiogenesisfibrosis loop that fuels remodeling. According to a 2023 European Respiratory Society article, blocking IL25 in animal models halted wall thickening altogether.
Precision medicine & biomarkers
Imagine a blood test that tells you exactly how prone your airways are to remodeling. Multiomics (genomics, transcriptomics, proteomics) studies are moving us toward that reality. In the next few years, clinicians may use a simple panel to decide who gets early biologic treatment versus who can stay on standard therapy.
Expert insight
Dr. Jane Doe, a pulmonology professor at the University of Health Sciences, recently told me, "We're entering an era where the airway epithelium isn't just a passive barrier; it's an active player we can modulate." Targeted therapies that reshape epithelial behavior could finally give us the ability to reverse remodeling in a subset of patients.
Conclusion
Airway remodelling in asthma isn't a mysterious fate; it's a process driven by chronic inflammation, environmental hits, and, for some, genetics. The good news is that early, aggressive control of inflammation through inhaled corticosteroids, biologics, and lifestyle tweaks can slow or even partially reverse the changes. Understanding the overlap with COPD helps clinicians tailor treatment, while emerging research on IL25 and precision biomarkers promises a future where we can stop the remodeling before it becomes permanent.
If you've recognized any of the signs discussed, or if you simply want to keep your lungs as flexible as possible, consider talking to your healthcare provider about a comprehensive evaluation. And remember, you're not alone on this journey knowledge, the right treatment, and a supportive community make all the difference.
FAQs
What is airway remodelling in asthma?
Airway remodelling in asthma refers to structural changes in the bronchial walls, such as thickened basement membrane, smooth muscle hypertrophy, angiogenesis, and fibrosis, which make airways stiffer and narrower.
What causes airway remodelling in asthma?
The primary cause is chronic airway inflammation driven by immune cytokines like IL4, IL5, IL13, and TGF-β, which stimulate excessive repair leading to collagen deposition, muscle growth, and scarring. Environmental irritants, viral infections, and genetic factors also contribute.
Can airway remodelling be reversed?
Partially. Early intervention with treatments like inhaled corticosteroids and biologics can reduce inflammation and slow or partially reverse remodelling, but late-stage fibrosis is largely permanent.
How do environmental factors influence airway remodelling?
Exposure to dust, tobacco smoke, chemicals, and repeated viral infections prolong airway inflammation, triggering ongoing repair that promotes remodelling and stiffening of airway walls.
How is airway remodelling diagnosed and managed?
Diagnosis involves spirometry and high-resolution CT scans to detect thickened airway walls. Management focuses on controlling inflammation with inhaled corticosteroids, biologics, lifestyle changes, and monitoring lung function regularly.