If youve ever noticed a painful, bluish lump around your belly button and wondered if its something serious, the short answer is: it could be umbilical endometriosis, and the most reliable way to get rid of it is with targeted treatment. Below youll find a straighttothepoint guide on symptoms, why it happens, and the treatment options doctors actually use from hormonal meds to surgical removal plus what to expect during recovery.
Whether youre dealing with a tiny bump that hurts every month or a larger nodule thats affecting your confidence, this article is here to give you clear, friendly answers and help you decide the best next step.
Quick Facts Overview
| Question | TL;DR Answer |
|---|---|
| Is it lifethreatening? | Rarely; usually benign but can cause chronic pain and, in very few cases, affect fertility. |
| Can it lead to infertility? | Only if pelvic endometriosis coexists; isolated umbilical lesions rarely impact fertility. |
| When to seek immediate care? | Sudden swelling, heavy bleeding, foul discharge, or rapid growth see the When to Seek Immediate Care section. |
These quick points are meant to give you immediate reassurance while you read on for the details.
Understanding the Condition
What Causes Umbilical Endometriosis?
There are two main ways this condition shows up:
- Primary (spontaneous) UE Endometrial tissue somehow implants in the umbilicus without any prior surgery. The exact mechanism is still under study, but theories include lymphatic spread or metaplasia of local cells.
- Secondary UE Happens after laparoscopic procedures, trocar site incisions, or umbilical hernia repairs. The surgical scar can act as a welcome mat for endometrial cells.
Hormonal fluctuations, especially estrogen spikes during the menstrual cycle, make the tissue swell and bleed, which is why the lump often feels worse right before or during periods.
Typical Symptoms & How to Spot Them
Most people notice a combination of the following:
- Painful swelling that intensifies with menstrual cycles.
- Darkred or bluish nodules you can find many online to compare.
- Discharge or bleeding from the belly button (rare but can happen).
- Itching or eczemalike changes that follow the same monthly rhythm.
If any of these sound familiar, youre not alone many patients initially brush these signs off as just a skin thing.
Diagnosis Toolbox (What the Doctor Looks At)
- Physical exam The doctor gently palpates the nodule and asks about the timing of pain.
- Umbilical endometriosis ultrasound A highfrequency probe shows a hypoechoic lesion with internal blood flow, helping to gauge depth.
- MRI or CT scan Used when theres suspicion of hidden pelvic disease.
- Biopsy / excisional pathology The gold standard; a tiny tissue sample confirms endometrial glands outside the uterus.
According to a recent review, ultrasound correctly identifies the lesion in about 85% of cases, making it the firstline imaging test ().
Best Treatment Options
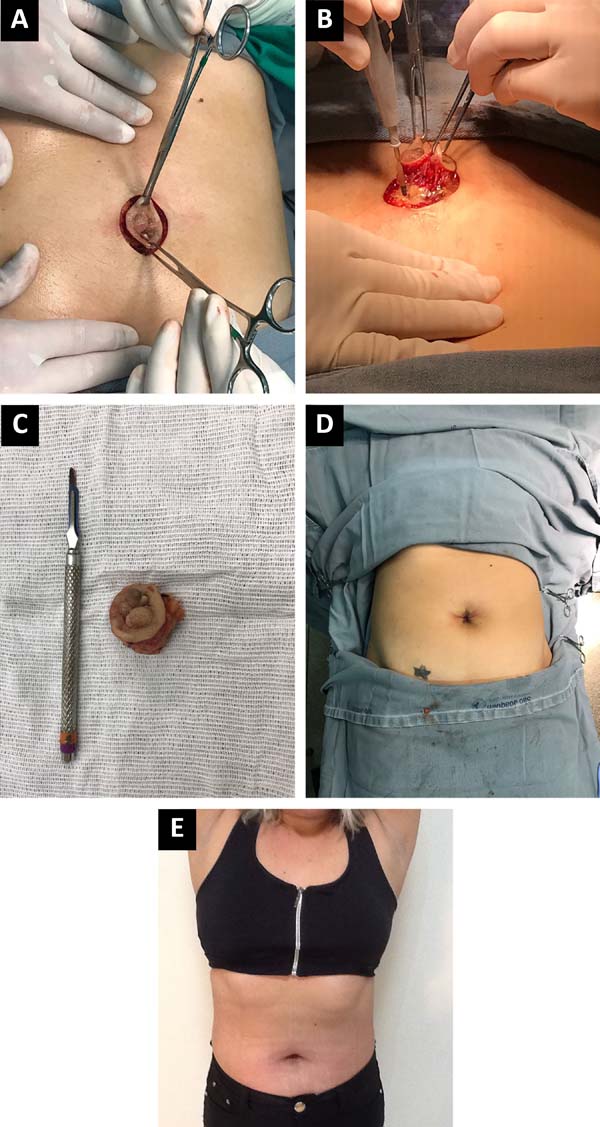
Surgical Treatment The Gold Standard
| Suboption | What It Involves | Pros | Cons |
|---|---|---|---|
| Wide local excision | Remove the lesion with a cuff of healthy tissue. | Highest cure rate, low recurrence (5%). | Small scar, risk of wound infection. |
| Laparoscopic excision | Endoscopic removal + inspection of pelvis. | Minimal incision, checks for hidden pelvic lesions. | Requires general anesthesia, longer setup. |
| Omphalectomy (complete navel removal) | Entire umbilicus removed; reconstruction later. | Guarantees removal of deep tissue. | Cosmetic impact; may need graft. |
Most surgeons consider surgical removal the definitive and safest approach. The procedure is usually done under local or general anesthesia, lasting less than an hour. After the nodule is out, a pathologist confirms that all endometrial tissue has been excised.
What to Expect Surgery Recovery Timeline
- Day 01: Observation, pain control, wound dressing.
- Day 27: Light activity; keep the area dry; avoid heavy lifting.
- Week 24: Stitches (if nonabsorbable) are removed; gentle scar massage can help.
- Month 13: Full return to normal activities; followup ultrasound may be scheduled to ensure no residual tissue.
Patients typically report a rapid drop in painoften within 48 hoursonce the lesion is gone.
Medical (Hormonal) Management When Surgery Isnt Immediate
| Medication | Mechanism | Typical Course | Success Rate |
|---|---|---|---|
| Progesterone (e.g., medroxyprogesterone acetate) | Suppresses ectopic endometrial growth. | 36months. | Partial symptom relief (~40%). |
| Danazol | Antiandrogenic, reduces estrogen. | 24months. | Variable; more side effects. |
| Norethisterone | Progestin, cyclic dosing. | 39months. | Moderate improvement. |
Hormonal therapy can shrink the nodule and ease pain, but it rarely eradicates the lesion completely. Thats why many clinicians prefer to use meds as a bridge to surgery or when a patient isnt a good surgical candidate.
When to Combine Hormones + Surgery
If the nodule is large or located deep within the tissue, a short course of progesterone may soften it, making the surgical excision cleaner and the scar smaller. Similarly, patients who already have pelvic endometriosis often benefit from systemic hormonal treatment while they wait for definitive surgery.
Supportive & Symptomatic Care
- Pain relief: NSAIDs or acetaminophen as needed.
- Topical heat: Warm compresses can soothe the area before a doctors visit.
- Scar care: Silicone gels or sheets after the incision heals.
- Lifestyle tips: Regular gentle exercise and stressreduction (yoga, breathing exercises) may help keep estrogen levels more balanced.
Frequently Asked Questions
Is umbilical endometriosis dangerous?
Its rarely lifethreatening, but it can cause chronic pain and, if left untreated, may signal hidden pelvic disease that could impact fertility. The lesion itself is benign in the overwhelming majority of cases.
Can umbilical endometriosis cause infertility?
Isolated umbilical lesions seldom affect fertility. However, many women with an umbilical nodule also have pelvic endometriosis, which can make it harder to conceive. A thorough pelvic workup is recommended if youre planning a family.
What does the recovery after umbilical endometriosis surgery look like?
Most people feel back to normal within 24weeks, with full activity returning after 36weeks. Scarring is usually minimal, especially with laparoscopic techniques.
Will the lesion come back after treatment?
Recurrence after complete excision is lowabout 5%. Hormonal therapy alone, however, has a higher relapse rate because the tissue isnt removed.
Do I need an ultrasound before treatment?
Yes. An clarifies the size and depth of the nodule, guiding the surgeon on the best approach.
Real World Experiences
Case Study 1: Maria, 32, noticed a bluish bump that hurt every month. After an ultrasound confirmed umbilical endometriosis, she underwent laparoscopic wide excision. Pain vanished within two days, and the scar faded after three months. I finally felt like my body was back to normal, she told me.
Case Study 2: Jenna, 27, had a small nodule but wanted to avoid surgery because she was planning a pregnancy. Her doctor started her on lowdose progesterone for four months. The pain lessened, but the nodule persisted, so she later chose a minimally invasive excision. Recovery was smooth, and shes now pregnant.
These stories illustrate that while every journey is unique, most people find reliefwhether through surgery, hormones, or a combination.
Making the Decision
| Decision Point | Considerations |
|---|---|
| Confirm diagnosis | Physical exam, ultrasound, biopsy. |
| Assess symptom severity | Keep a pain diary, note menstrual correlation. |
| Fertility goals | Discuss pelvic workup if trying to conceive. |
| Choose treatment route | Firstline surgery vs. hormonal bridge. |
| Plan postop care | Wound care, followup imaging, scar management. |
| Seek second opinion | Especially for rare or recurrent cases. |
Take your time with each step. Ask your doctor to explain why they recommend a particular approach, and dont hesitate to get another perspective if something feels off.
Conclusion
Umbilical endometriosis may feel like a mysterious bellybutton bump, but the good news is that effective, evidencebacked treatments exist. If youre dealing with pain, cyclical swelling, or discharge, a focused ultrasound and surgical excision usually give the best, longestlasting relief, while hormonal therapy can serve as a useful bridge or adjunct. Understanding the conditions cause, the realistic recovery timeline, and the modest risk of recurrence empowers you to make an informed choicewhether you opt for surgery, medication, or a combination.
Whats your experience with umbilical endometriosis? Have you tried a treatment that worked (or didnt)? Share your story in the comments, and if you have any lingering questions, feel free to ask. Were all in this together.
FAQs
Can umbilical endometriosis be treated without surgery?
Hormonal therapy can reduce pain and shrink the nodule, but it rarely eliminates the tissue completely. Most doctors recommend surgery for a definitive cure, using medication as a bridge when needed.
How long does recovery take after umbilical endometriosis excision?
Typical recovery is 2‑4 weeks for light activity, with full return to normal tasks in 3‑6 weeks. Stitches are usually removed after 2 weeks, and pain diminishes within days.
Will hormonal therapy prevent recurrence after surgery?
Post‑operative hormonal suppression can lower the chance of recurrence, especially if pelvic endometriosis is present, but the lowest relapse rates (≈5%) are seen after complete surgical excision alone.
Is umbilical endometriosis linked to fertility issues?
Isolated umbilical lesions seldom affect fertility. However, many women also have pelvic endometriosis, which can impact conception, so a pelvic evaluation is advised if you plan a pregnancy.
What signs indicate I should see a doctor right away?
Seek immediate care for sudden swelling, heavy bleeding, foul discharge, rapid growth of the nodule, or severe pain that doesn’t follow the menstrual cycle.