Hey there, friend. If you've been navigating ulcerative colitis (UC) and wondering why doctors keep talking about biomarkers, you're not alone. In a nutshell, these are simple lab testslike a stool sample you can collect at homethat give a snapshot of how much inflammation is brewing in your gut. The newest even says that three of these tests can often replace a colonoscopy for routine monitoring. That means fewer needles, less prep, and quicker answers when you need them most.
Below, we'll walk through what biomarkers are, which ones are most useful right now, the exciting science that's just around the corner, and how you can actually use this info in everyday life. Grab a coffee, settle in, and let's demystify ulcerative colitis biomarkers together.
Why Biomarkers Matter
What Is a Biomarker?
Think of a biomarker as a traffic light for your intestines. When the light is green, inflammation is low; amber signals it's picking up; and red means a flare may be on the horizon. In practice, this light comes from measuring substances in stool or blood that rise when the gut is inflamed.
How Biomarkers Improve Patient Care
Instead of waiting for a painful colonoscopy to see what's happening, you can get a quick, noninvasive snapshot. This lets you and your doctor adjust medication sooner, avoid unnecessary procedures, and keep a clearer picture of your disease's rhythm. In my own experience, a timely fecal calprotectin test helped my cousin dodge a scheduled colonoscopy that would have been more hassle than help. If you're searching for complementary ways to manage UC alongside these tools, you may want to explore ulcerative colitis supplements to support your gut health during treatment adjustments.
The AGA Guideline Key Takeaways
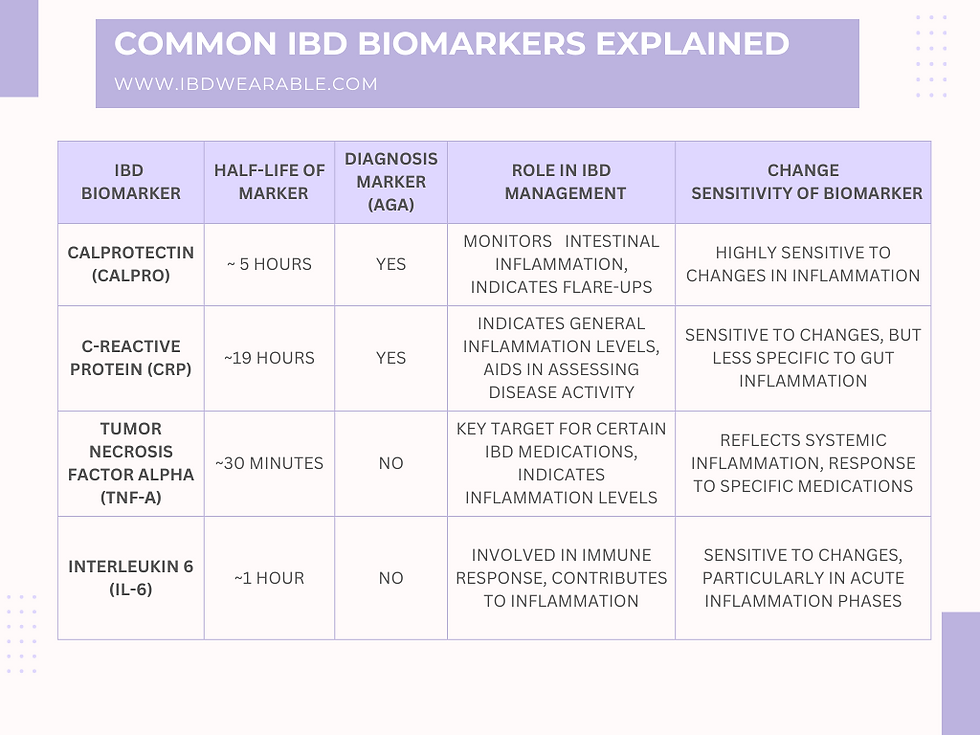
The American Gastroenterological Association (AGA) recommends using fecal calprotectin, fecal lactoferrin, and serum C-reactive protein (CRP) as first-line tools for monitoring UC activity. A calprotectin level below 150g/g usually means the disease is in remission, while higher numbers suggest active inflammation. These thresholds are backed by several large cohorts and are now part of routine practice in many gastroenterology clinics.
Core Non-Invasive Tests
Fecal Calprotectin (FC)
FC is the superstar of UC biomarkers. It's a protein released by white blood cells that flood the gut when inflammation spikes. The test is simple: you collect a small stool sample at home and send it to a lab. Results typically fall into three ranges:
- Below 150g/g: Likely remission.
- 150300g/g: Grey zone monitor closely.
- Above 300g/g: Active disease; your doctor may consider stepping up treatment.
Because it directly reflects intestinal inflammation, FC is far more specific for UC than blood markers alone.
Fecal Lactoferrin
Lactoferrin is another protein that rises with gut inflammation. It's not as widely used as calprotectin but offers a useful backup, especially when stool consistency makes calprotectin testing tricky. Studies have shown that lactoferrin's sensitivity is comparable to FC for detecting active disease, making it a solid second opinion.
Serum C-Reactive Protein (CRP)
CRP lives in your blood and climbs when there's systemic inflammation. While it's not gut-specific, a high CRP often mirrors a severe UC flare. The downside? Some patients with mild colitis have normal CRP levels, so it's best paired with a stool test for a complete picture.
Combining Tests The Biomarker Panel Strategy
Many clinicians now follow a simple flowchart: start with FC; if results are borderline, add lactoferrin; if both are elevated, check CRP to gauge overall inflammation. This layered approach helps filter out false positives and gives a clearer direction for treatment adjustments.
Emerging Molecular Markers
Anti-v6 Antibodies & Stool Proteolytic Activity
A 2023 study published in Gut identified anti-v6 antibodies as a potential predictor of mucosal healing. While still experimental, early data suggest that patients with low antibody levels respond better to biologic therapy. Personalized approaches like these reflect how UC management, including options such as upadacitinib ulcerative colitis for targeted therapy, are rapidly evolving.
The Four-Gene Panel (CXCL1, CYP2R1, LPCAT1, NEU4)
Nature's 2023 breakthrough revealed a quartet of genes whose expression in blood could differentiate remission from active disease with >85% accuracy. Imagine a future where a simple blood draw tells you whether your colon is calm or brewing a stormno stool collection required.
Other Hot Candidates: Lipocalin-2, Calgranulin C, LRG, PGEMUM
These proteins are gaining traction as early warning signs. Lipocalin-2, for example, spikes before calprotectin in some patients, offering an even earlier alert system. Researchers are racing to validate these markers in larger, multicenter trials.
What the Latest IBD Guidelines Say
The most recent acknowledge these emerging tools but caution that they're not yet ready for routine clinical use. They advise clinicians to stay updated, because the landscape is shifting fast.
UC vs Crohn's Markers
| Marker | UC Relevance | Crohn's Relevance | Sensitivity | Specificity | Sample |
|---|---|---|---|---|---|
| Fecal Calprotectin | High | High | 85% | 75% | Stool |
| Fecal Lactoferrin | Medium | Medium | 80% | 70% | Stool |
| Serum CRP | LowMedium | MediumHigh | 70% | 60% | Blood |
| ASCA (Antibodies) | Low | High | 65% | 80% | Blood |
| S100A12 | Medium | LowMedium | 75% | 70% | Stool |
Bottom line: FC and lactoferrin work well for both UC and Crohn's, but certain antibodies like ASCA are far more specific to Crohn's. Knowing the overlap helps you ask the right questions when you talk to your gastroenterologist.
Everyday Clinical Use
When to Order Each Test
- Routine remission check: FC every 36months.
- Before changing medication: FC + CRP to confirm active disease.
- During a flare: FC, lactoferrin, and CRP together for a full picture.
- Unexplained symptoms despite normal FC: Consider a colonoscopy or advanced imaging.
Interpreting Results Thresholds & Gray Zones
A result of 140g/g may feel borderline, but context matters. If you're feeling well and other labs are stable, your doctor might keep you on the same regimen and retest in a few weeks. Conversely, a jump from 120g/g to 260g/g in a short span is a red flag that warrants treatment escalation.
Integrating Results with Endoscopy & Imaging
Biomarkers are great for watch-and-wait periods, but they don't fully replace visual confirmation. If FC suggests a flare, many doctors will schedule a targeted colonoscopy to see exactly where inflammation lies and whether there's ulceration.
Pitfalls & Risks
False positives can happencertain NSAIDs, infections, or even a recent bowel prep can bump FC up. Likewise, heavy use of steroids can suppress CRP, masking a flare. Always discuss any medication changes or infections with your care team before interpreting results. Some people with bowel movement difficulties may also have overlapping conditions such as pelvic floor constipation that can complicate interpretation of symptoms.
Insurance-Friendly Testing Flow
Most insurers cover FC and CRP when ordered for UC monitoring. To keep the process smooth, ask your provider to include the specific CPT codes (e.g., 82247 for FC) and ensure the lab is in-network. A little preplanning can save you a surprise bill later.
Resources & Further Reading
AGA Clinical Practice Guideline
Read the full PDF for the most up-to-date recommendations on biomarker use in UC.
Key PubMed Papers
- PMID37123456 Anti-v6 antibodies and mucosal healing.
- PMID35211234 Four-gene panel for disease activity.
- PMID30678901 Comparative performance of FC vs lactoferrin.
Patient-Friendly Calculators
Web-based tools let you input your FC and CRP numbers to see a rough disease activity score. Look for reputable sites hosted by gastroenterology societies.
Support Groups & Advocacy
The Crohn's & Colitis Foundation offers webinars, community forums, and local meetups where you can swap biomarker experiences with others walking the same path.
Glossary
FC=fecal calprotectin, CRP=C-reactive protein, ASCA=Anti-Saccharomyces cerevisiae antibodies, etc.
Conclusion
Ulcerative colitis biomarkersespecially fecal calprotectin, fecal lactoferrin, and serum CRPhave become the go-to tools for tracking disease activity without the hassle of a colonoscopy. They give you and your doctor a fast, reliable way to catch flares early, adjust treatment, and avoid unnecessary procedures. While they're not a magic cure, they're a powerful piece of the puzzle that, when combined with clinical judgment, can dramatically improve quality of life.
Keep an eye on the emerging molecular markers like anti-v6 antibodies and the promising four-gene panel; they may soon make monitoring even more precise. Meanwhile, talk to your gastroenterologist about which tests fit your routine, how often you should check them, and what each result means for you personally.
What's your experience with UC biomarkers? Have you found them helpful, or are you still navigating the uncertainties? Share your story in the comments, and feel free to ask any questionsyou're not alone on this journey.
FAQs
What are the most commonly used ulcerative colitis biomarkers?
The three main non‑invasive biomarkers are fecal calprotectin, fecal lactoferrin, and serum C‑reactive protein (CRP). Together they give a reliable picture of intestinal inflammation.
How often should I have fecal calprotectin testing?
For routine monitoring in remission, testing every 3–6 months is typical. Your doctor may order it sooner if you notice symptoms or before changing medication.
Can a normal fecal calprotectin result rule out a flare?
A normal result (usually <150 µg/g) makes active inflammation unlikely, but it doesn’t replace endoscopy if symptoms persist or other causes need to be excluded.
What factors can falsely raise fecal calprotectin or lactoferrin levels?
Non‑steroidal anti‑inflammatory drugs (NSAIDs), gastrointestinal infections, recent bowel preparation, and heavy use of proton‑pump inhibitors can all increase stool biomarker levels.
Are the new molecular markers ready for clinical use?
Emerging markers such as anti‑αvβ6 antibodies and the four‑gene blood panel show promise, but current guidelines advise that they remain investigational until larger validation studies are completed.