If your thyroid is the factory that makes the hormones T3 and T4, primary hypothyroidism means the factory itself is broken. There are three main flavorsautoimmune (Hashimotos), postsurgical/iodinedeficiency, and congenital/postpartumeach with its own lab fingerprint and treatment tricks.
Knowing which type you have helps you read your labs (high TSH, low T3/T4), pick the right dose of levothyroxine, and avoid unnecessary scares. Let's break down the three types, see how they differ from secondary or tertiary hypothyroidism, and explore what the latest guidelines say.
Primary vs Others
What is the difference between primary, secondary, and tertiary hypothyroidism?
In a nutshell, primary hypothyroidism starts in the thyroid gland itself, secondary originates in the pituitary gland, and tertiary stems from the hypothalamus. The organ that fails determines the lab pattern.
Quick Comparison Table
| Condition | Problem Area | TSH | Free T4 | Free T3 |
|---|---|---|---|---|
| Primary | Thyroid gland | High | Low | Low |
| Secondary | Pituitary gland | Low/Normal | Low | Low |
| Tertiary | Hypothalamus | Low/Normal | Low | Low |
How do lab values pinpoint primary hypothyroidism?
When the thyroid can't make enough hormone, the pituitary screams "more!" and lifts TSH. So you'll usually see a high TSH with low free T4 (and often low free T3). That pattern is the hallmark that doctors use to label it primary.
Main Types
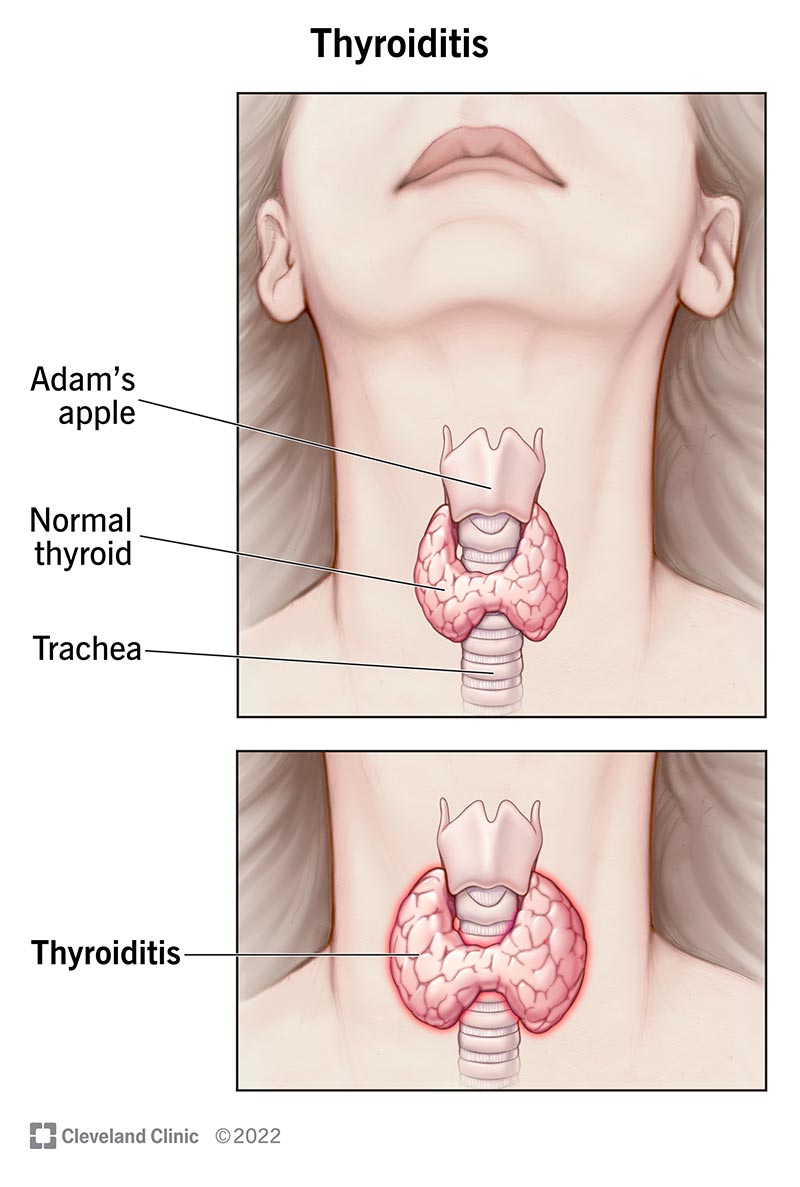
1 Autoimmune (Hashimotos) Thyroiditis
Hashimotos is the most common cause of primary hypothyroidism in the United States. It's a friendlyfire situation where the immune system attacks the thyroid, slowly burning it out over years.
Typical cause & risk factors
- Family history of autoimmune disease
- Female gender (about 89 times more common)
- Other conditions such as type 1 diabetes, celiac disease, or rheumatoid arthritis
Lab hallmark
High TSH, low free T4, plus positive antiTPO (thyroid peroxidase) or antiTG (thyroglobulin) antibodies. According to studies, antibodies are present in more than 90% of confirmed cases.
Realworld story
Jane, 38, felt unusually sluggish during her annual checkup. Her doctor ordered a simple TSH test; the result was 7.2 IU/mL (normal up to 4.0). A followup panel showed high antiTPO antibodies, confirming Hashimotos. Within weeks of starting lowdose levothyroxine, her energy bounced back and the brain fog lifted.
2 IodineDeficiency / PostSurgical / RadioiodineInduced
Not all thyroid trouble comes from the immune system. If the gland is missing (surgical removal) or starved of iodine, it simply can't produce T3/T4.
Iodine's role
Iodine is the raw material for thyroid hormone synthesis. In regions where soil iodine is low, diets often lack enough, leading to a slowly progressive hypothyroidism.
Postsurgical and radioiodine scenarios
Patients who have undergone total thyroidectomy for cancer or nodular disease, or who received radioactive iodine therapy, will be thyroidless and require lifelong hormone replacement.
Patient vignette
Mark, 52, was diagnosed with papillary thyroid carcinoma. After a total thyroidectomy and radioactive iodine ablation, his surgeon explained he'd need daily levothyroxine for the rest of his life. He now checks his TSH every 6 months and feels just like his old self.
3 Congenital & Postpartum
Some babies are born with a thyroid that never fully develops (congenital). Others, especially new moms, experience a sudden autoimmune flare that mimics Hashimotos but shows up after delivery.
Why newborn screening matters
In most countries, every newborn gets a heelstick blood test for TSH. Early detection prevents irreversible neurodevelopmental delays.
Postpartum flareup
Laura, 30, noticed overwhelming fatigue and hair loss three weeks after giving birth. A simple blood workup revealed a TSH of 9.5 IU/mL and low free T4. Her doctor diagnosed postpartum hypothyroidism, started a low dose of levothyroxine, and her symptoms receded within a couple of months.
Diagnosis Guide
What labs do I need?
The thyroid workup starts with TSH. If it's high, the next step is free T4 (and sometimes free T3) to see how much hormone is actually circulating. Antibody panels (antiTPO, antiTG) help confirm an autoimmune cause. In iodinedeficiency regions, a urinary iodine concentration can be informative.
Stepbystep flowchart
| Step | Test | Interpretation |
|---|---|---|
| 1 | TSH | High suspect primary hypothyroidism |
| 2 | Free T4 (Free T3) | Low confirms overt disease; normal with high TSH = subclinical |
| 3 | AntiTPO / AntiTG | Positive = autoimmune (Hashimotos) |
| 4 | Ultrasound or Radioiodine Uptake | Used when nodules or surgical history present |
When is imaging needed?
Most primary hypothyroidism is diagnosed with blood work alone. Imaging becomes relevant if the doctor suspects nodules, thyroiditis with enlargement, or if you've had a thyroidectomy and need to check residual tissue.
Subclinical primary hypothyroidism
That's the borderline stageTSH is elevated, but free T4 and free T3 stay within normal limits. The debate about treatment is still alive, but many endocrinologists recommend therapy if TSH is above 10 IU/mL or if you have symptoms, cardiovascular risk, or are pregnant.
Treatment Options
Standard levothyroxine monotherapy
Levothyroxine (synthetic T4) is the goldstandard. Most people start with 1.6 g/kg/day and then adjust based on followup TSH. Take it on an empty stomach, ideally 30 minutes before breakfast, to maximize absorption.
When is combination T4+T3 considered?
About 510% of patients on levothyroxine alone still feel fatigued despite a normal TSH. A small subset benefits from adding a shortacting T3 (liothyronine). It's a personalized decision, usually tried after a few months of stable T4 dosing.
Beyond medication: Lifestyle tweaks
- Diet: Selenium (found in Brazil nuts) can modestly reduce antiTPO titers.
- Stress management: Chronic stress may aggravate autoimmune activity, so yoga or mindfulness can help.
- Calcium & iron: Avoid taking levothyroxine within 4 hours of calcium or iron supplements; they interfere with absorption.
Comparison of treatment nuances
| Type | Firstline | Typical Dose | Special Considerations |
|---|---|---|---|
| Autoimmune | Levothyroxine | 1.6 g/kg/day | Monitor antibodies; consider selenium |
| Iodinedeficiency / Postsurgical | Levothyroxine | Adjust to TSH target | Check calcium/vitamin D status |
| Congenital / Postpartum | Levothyroxine | Weightbased, reevaluate frequently | Tight TSH targets in pregnancy |
Risks & Benefits
Overreplacement signs
Too much hormone can feel like having a caffeine overdose: rapid heartbeat, anxiety, insomnia, and even bone loss over time. Regular TSH checks protect against this.
Underreplacement clues
If you still feel sluggish, gain weight, or notice dry skin despite a normal TSH, ask your doctor for a free T4 repeat. Sometimes the target range needs tweaking.
Pregnancy considerations
During pregnancy, the placenta demands more thyroid hormone. The American Thyroid Association recommends a TSH target below 2.5 IU/mL in the first trimester. Your doctor may increase your levothyroxine dose by 30% as soon as you confirm pregnancy.
Drug interactions to watch
Calcium carbonate, iron sulfate, certain cholesterollowering drugs (e.g., cholestyramine), and protonpump inhibitors can all lower levothyroxine absorption. Space them out by at least 4 hours.
FAQ Highlights
What are the three types of hypothyroidism?
They're the autoimmune (Hashimotos), iodinedeficiency/postsurgical (including radiation), and congenital/postpartum forms.
How does primary differ from secondary?
Primary starts in the thyroid itself and shows high TSH with low T4/T3. Secondary originates in the pituitary, so TSH is low or inappropriately normal while T4/T3 are low.
Can primary hypothyroidism be cured?
Unfortunately, the gland's damage is usually permanent. Treatment focuses on replacing the missing hormones and managing symptoms.
What does subclinical hypothyroidism mean?
It's a mild form where TSH is elevated but T4/T3 stay normal. Many never need medication, but some benefit from early treatment, especially if TSH > 10 IU/mL or you're pregnant.
Is Hashimotos the most common cause?
Yesstudies in the United States show it accounts for roughly 70% of primary hypothyroidism cases.
What T3 and T4 levels indicate primary hypothyroidism?
Typical free T4 ranges are 0.81.8 ng/dL; values below ~0.8 suggest overt disease when TSH is high. Free T3 is less often measured but falls below ~2.3 pg/mL in many untreated patients.
Should I get tested for secondary hypothyroidism?
If you have a history of pituitary surgery, radiation, or known pituitary tumors, your doctor may order a pituitary panel alongside thyroid tests.
Helpful Resources
Downloadable cheat sheet
Click the link below to get a printable PDF that breaks down TSH, T4, and T3 values, plus a quick dosing guide for levothyroxine. Keep it on your fridge for an ataglance reminder.
Interactive dose calculator
Use the calculator to estimate your starting dose based on weight, age, and pregnancy status.
Trusted reference list
- Healthline Hashimotos overview
- Cleveland Clinic Hypothyroidism basics
- NCBI Subclinical hypothyroidism review
- American Family Physicians Treatment algorithms
- American Thyroid Association Clinical practice guidelines
Conclusion
Understanding the three flavors of primary hypothyroidismautoimmune, iodinedeficiency/postsurgical, and congenital/postpartumhelps you read your labs, pick the right treatment, and avoid unnecessary scares. Whether you're newly diagnosed or have been living with the condition for years, regular TSH checks, personalized medication, and a few lifestyle tweaks keep the thyroid clock ticking smoothly. Got more questions? Share your experience in the comments, or reach out to a trusted endocrinologistyou deserve clear answers and a healthy, energetic life.
For more on choosing the right thyroid replacement and the differences between preparations, see Armour vs levothyroxine for a comparison that may help when standard levothyroxine doesn't fully relieve symptoms.
FAQs
What are the main types of primary hypothyroidism?
The main types are autoimmune (Hashimoto’s), iodine-deficiency/post-surgical, and congenital/post-partum hypothyroidism.
How is primary hypothyroidism diagnosed?
It is diagnosed with blood tests showing high TSH and low free T4, sometimes with positive thyroid antibodies.
Is Hashimoto’s the most common cause of primary hypothyroidism?
Yes, Hashimoto’s thyroiditis is the most common cause of primary hypothyroidism in the United States.
Can primary hypothyroidism be cured?
No, it is usually permanent and requires lifelong hormone replacement therapy.
What is subclinical primary hypothyroidism?
It is a mild form where TSH is elevated but free T4 and T3 are normal, often not requiring immediate treatment.