Standard Treatment Overview
FirstLine Antibiotics for Bacterial Meningitis
When a child is diagnosed with bacterial meningitis, speed is everything. The most common regimen starts with a combination of ampicillin and a thirdgeneration cephalosporin such as ceftriaxone or cefotaxime. This duo blankets the usual suspectsGroupB Streptococcus, Streptococcus pneumoniae, and Neisseria meningitidis. If theres any hint that S. pneumoniae might be resistant, doctors add vancomycin to the mix.
When Antivirals Are Needed
Viral meningitis, especially from herpes simplex virus, is far less lethal, but it still needs attention. In those rare cases, acyclovir is given intravenously. Most viral infections, however, are handled with supportive carehydration, fever reducers, and rest.
Do Steroids Help?
Many pediatric specialists give a single dose of dexamethasone right before the first antibiotic. The idea is to calm the inflammation around the brain and spinal cord. Recent suggests dexamethasone is most useful when H. influenzae is suspected, but its not a blanket rule for every child.
Typical Dosing (per kilogram)
| Medication | Loading Dose | Frequency |
|---|---|---|
| Ampicillin | 200mg/kg | Every 6h |
| Cefotaxime | 100mg/kg | Every 6h |
| Vancomycin | 20mg/kg | Every 6h (adjusted by levels) |
| Dexamethasone | 0.6mg/kg | Single dose before antibiotics |
Nursing & Hospital Care
First Hours: What Happens After You Arrive?
The moment the ER team suspects meningitis, theyll start two things simultaneously: secure an IV line and draw blood for labs. Within an hour, a lumbar puncture is performedyes, that spinal tap youve heard about. Its the goldstandard test to confirm whether the culprit is bacterial, viral, or something else.
Nursing Management Essentials
- Vital signs every hour: fever spikes, blood pressure, and heart rate can hint at worsening infection.
- Neurological checks: nurses assess the childs level of consciousness, pupil reactions, and any new seizures.
- Fluid therapy: keeping the child hydrated helps the antibiotics circulate better and reduces the risk of kidney injury.
- Pain and fever control: acetaminophen or ibuprofen are given on a regular schedule, not just when the child cries.
- Family communication: nurses keep parents updated every shiftwhat meds are being given, why, and what to watch for at home.
PostAcute Care and Discharge Planning
After the infection is under control (usually 4872hours of IV antibiotics), the medical team decides whether the child can switch to oral antibiotics. This is a big reliefno more hospital drip, but it comes with a checklist:
- Ensure the child can keep oral meds down.
- Schedule a followup visit with a pediatric infectiousdisease specialist.
- Arrange hearing and developmental screeningmeningitis can sometimes leave subtle aftereffects.
Common Causes Overview
Bacterial Culprits by Age
Age is a strong predictor of the offending bug:
- Neonates (01month): GroupB Streptococcus, E. coli, and Listeria monocytogenes.
- Infants (15years): Streptococcus pneumoniae and Neisseria meningitidis dominate.
Viral Agents Most Often Seen
Enteroviruses rule the summer months, causing a milder, selflimited meningitis. Herpes simplex virus (HSV1 or HSV2) is rarer but dangerous; thats why the acyclovir safety net exists.
When to Think Beyond Bacterial and Viral
If the child has a compromised immune system, doctors will also look for fungal meningitis or tuberculosis. Those cases need completely different medicines and a longer treatment course.
Guideline Resources Download
Official PDFs You Can Keep at Hand
Downloading a concise, reputable guideline is like having a cheatsheet for emergencies. The American Academy of Pediatrics (AAP) released an updated that spells out dosage, fluid management, and when to add steroids. In the UK, the NHS publishes a short that can be printed as a quick reference.
SlideShare Style Quick Reference
If you love visual learning, the Management of Meningitis in Pediatrics Slideshare deck condenses the whole protocol into five slidesperfect for a bedside review or a study group.
How to Use the PDFs in Real Time
- Print the first page and tape it to the IV pole for rapid dose checks.
- Bookmark the PDF on your phone so you can pull it up while talking to the doctor.
- Share the file with other parents in your support group; knowledge spreads faster than germs.
Risks & Benefits
Why Prompt Treatment Saves Lives
When antibiotics are started within the first hour of suspicion, survival rates climb above 90% in highresource settings. Early therapy also slashes the chance of longterm complications like hearing loss, learning difficulties, or motor deficits.
Potential SideEffects to Watch
- Antibiotic reactions: rash, upset stomach, or in rare cases, Clostridioides difficile infection.
- Steroid concerns: temporary high blood sugar, especially in children with preexisting diabetes.
- IV line issues: infiltration or infection at the catheter site.
DecisionMaking Checklist for Families
Feeling overwhelmed? Bring these questions to the bedside:
- Why did you choose this specific antibiotic?
- Do we need steroids, and what are the risks for my child?
- When can we switch to oral medication?
- What followup tests are required after discharge?
Real World Stories
Case 1 Baby Emmas Close Call
Emma was eight months old when she developed a fever, irritability, and a bulging fontanelle. A swift lumbar puncture revealed GroupB Streptococcus. She received the standard ampicillinplusceftriaxone combo, plus a single dose of dexamethasone. Within three days, her fever melted away, and she was sent home on oral amoxicillin. Six weeks later, her pediatrician confirmed normal hearing and development. Parents say the cheatsheet PDF saved them from endless phone calls to the ER.
Case 2 Liams Viral Meningitis
Liam, a lively fouryearold, showed a stiff neck and mild fever. The team performed a lumbar puncture, and the lab showed a viral pattern. No antibiotics were givenonly fluids, acetaminophen, and a lot of cuddles. He bounced back in a week. Liams mother highlights how the viral vs. bacterial distinction prevented unnecessary drug exposure.
Conclusion
Understanding the treatment of meningitis in pediatric patients isnt just a medical checklist; its a roadmap that empowers you as a parent. Quick, evidencebased antibiotics, thoughtful nursing care, and clear communication can turn a terrifying emergency into a manageable journey. Remember to download the trusted , keep a symptom diary, and never hesitate to ask the why behind every decision. If this guide helped you feel a little more prepared, share it with friends, leave a comment with your own story, or reach out with questionsyour experience might be the lifeline another family needs.
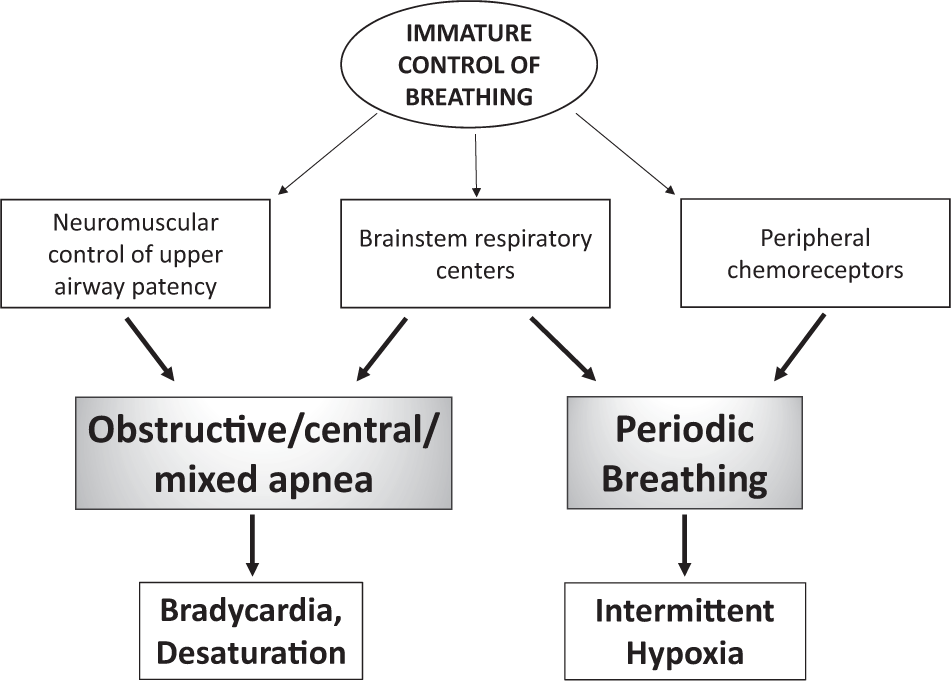
For parents concerned about related symptoms like infant apnea, discussing breathing patterns alongside meningitis evaluation can be important, especially in very young infants.
FAQs
What is the first-line treatment for bacterial meningitis in children?
The first-line treatment typically involves intravenous ampicillin plus a third-generation cephalosporin, such as ceftriaxone or cefotaxime. Vancomycin is added if there is concern for resistant Streptococcus pneumoniae.
When are antivirals used in pediatric meningitis treatment?
Antivirals like intravenous acyclovir are used mainly for suspected or confirmed viral meningitis caused by herpes simplex virus, while most viral meningitis cases require supportive care only.
What role do steroids play in treating pediatric meningitis?
A single dose of dexamethasone is often given before antibiotics to reduce inflammation, especially if Haemophilus influenzae is suspected; however, steroids are not universally used for every child.
What key nursing care is essential for children with meningitis?
Nursing care focuses on hourly vital sign and neurological monitoring, fluid management, pain and fever control, and clear communication with the family about treatment progress and home care.
How long is antibiotic therapy for bacterial meningitis in children?
The duration varies by pathogen but generally ranges from 7 to 21 days, with shorter courses for uncomplicated cases and longer for complicated infections like brain abscess or ventriculitis.