Feeling uneasy about bleeding risks or simply curious why cirrhosis drags your platelets down? Lets skip the jargon, look at realworld options, and give you a clear roadmap you can discuss with your doctor right now.
Why Platelets Drop
What causes thrombocytopenia in cirrhosis?
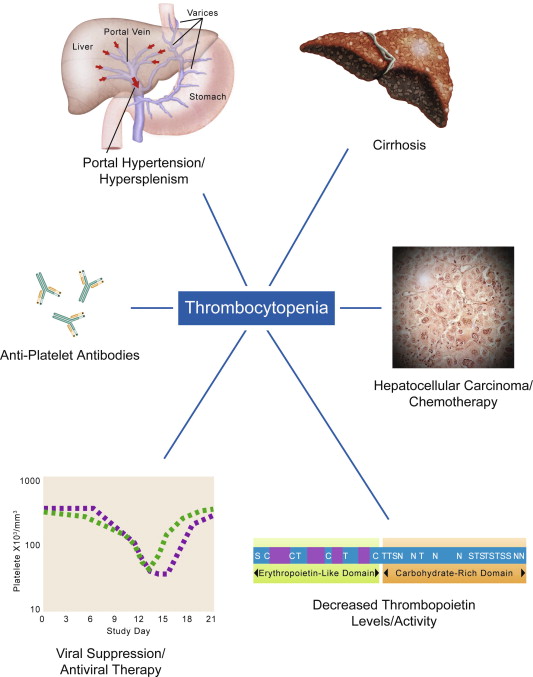
In cirrhosis the livers ability to produce thrombopoietin (the hormone that tells bone marrow to make platelets) drops dramatically. At the same time, portal hypertension often enlarges the spleen, and the spleen starts hoarding plateletsthink of it as a platelet warehouse that never ships them back into circulation.
How does portal hypertension affect platelets?
When blood pressure builds up in the portal vein, blood backs up into the spleen, causing it to swell. A bigger spleen traps more platelets, so the count you see on a lab test looks lower than whats actually being produced. A quick case study: John, 58, with portal hypertension, had a platelet count of 70K/L despite a healthy bone marrow.
Why is low platelet count common in endstage liver disease?
Studies show that 4555% of patients with endstage liver disease have platelets below 150K/L. The combination of reduced thrombopoietin, splenic sequestration, and sometimes bonemarrow suppression creates a perfect storm for thrombocytopenia.
Is low platelet count always dangerous?
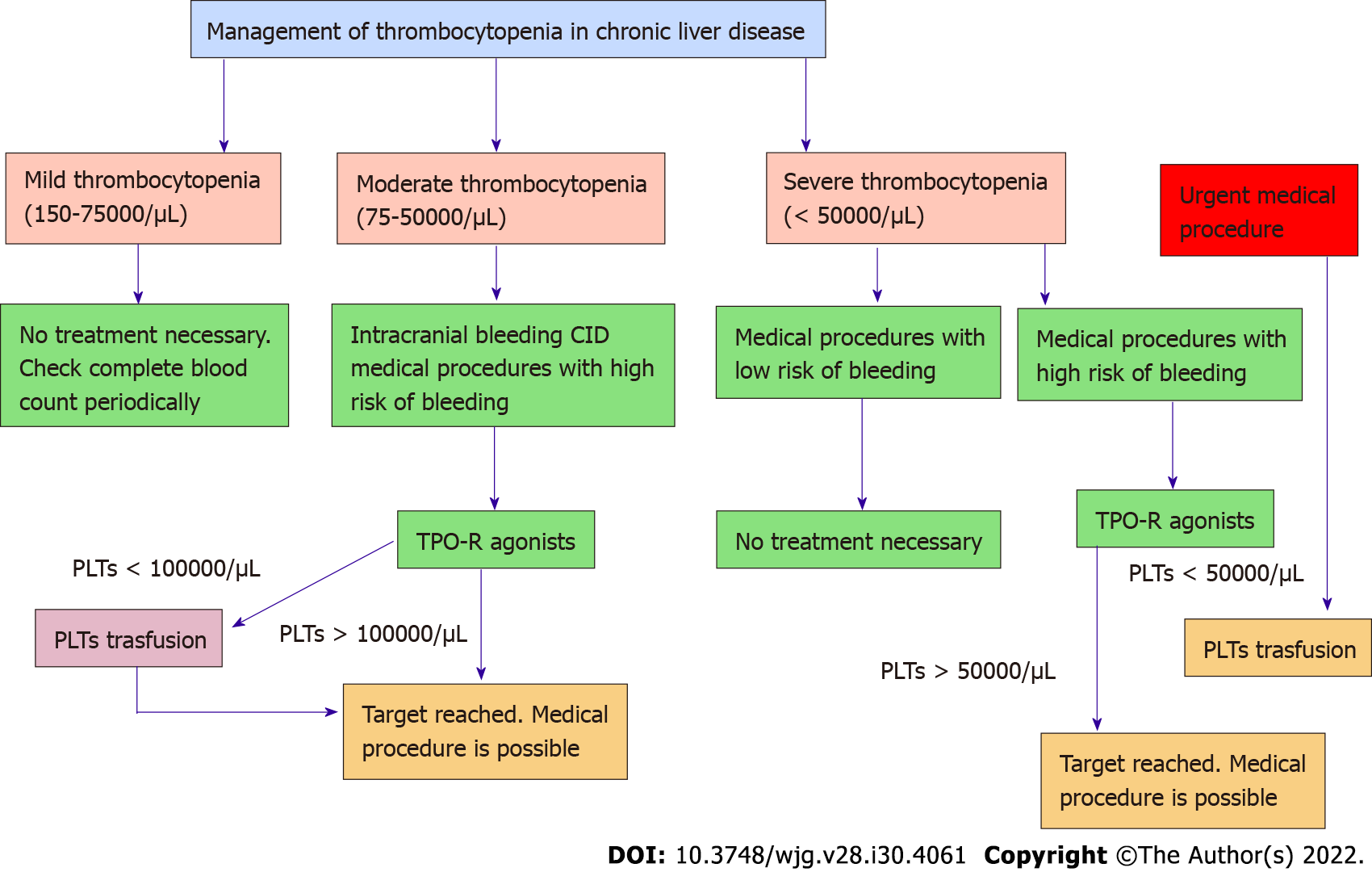
Not necessarily. Clinical thrombocytopenia refers to when the low count actually leads to bleeding problems. Many patients with counts around 80100K/L never experience a bleed. However, thresholds matter when you need surgery or an invasive procedureusually we aim for at least 50K/L for lowrisk workups and 7080K/L for higherrisk interventions.
Diagnosing Low Platelets
What is a normal platelet count in cirrhosis?
In a healthy adult, platelets range from 150400K/L. In cirrhosis, the normal range shifts down to roughly 80150K/L. Below 80K/L, most clinicians start to get concerned about bleeding.
When should I get a platelet count checked?
Routine monitoring every 36months is a solid rule of thumb, especially if you have ChildPugh class B or C disease. If you notice bruising, nosebleeds, or gum bleeding, call your hepatologist and ask for an immediate labs check.
How is thrombocytopenia confirmed?
The basic panel includes platelet count, mean platelet volume (MPV), PT/INR, and a liver function panel. Imagingusually an abdominal ultrasoundhelps us see if the spleen is enlarged. Together, these clues tell us whether the low count stems from reduced production, splenic sequestration, or another cause.
Can other conditions mimic low platelets?
Absolutely. Viral infections (like hepatitis C), certain medications (e.g., betablockers), autoimmune diseases, and even vitamin deficiencies can lower platelets. A quick checklist can help rule out these culprits before we focus on liverrelated solutions.
Treatment Options
Pharmacologic therapies
When it comes to medication, two oral thrombopoietinreceptor agonists (TPORAs) have become the backbone of modern care:
- Avatrombopag (Doptelet) FDAapproved in 2020 for patients with chronic liver disease undergoing invasive procedures. It raises platelets within 510 days and has a relatively low risk of blood clots.
- Lusutrombopag (Mulpleta) Works similarly but can be given for up to 7 days before a planned procedure, offering a onestop boost.
Both drugs are taken orally, which makes them far more convenient than repeated platelet transfusions. Speaking of transfusions, theyre still the gold standard for massive bleeds or when you need an immediate bumpjust remember they carry risks like alloimmunization and fluid overload.
Some clinicians also experiment with adjuncts such as lowdose danazol (an androgen) or even splenic radiation, but the evidence is limited. Natural supplements like vitaminK or folate are safe but usually wont raise platelets enough on their own.
Procedural & surgical options
If medication isnt enough, the next tier often involves the spleen:
| Procedure | How it works | Success Rate | Key Risks |
|---|---|---|---|
| Partial splenic embolisation (PSE) | Block blood flow to part of the spleen, reducing its platelettrapping capacity. | 7085% achieve >30K/L rise. | Postembolisation pain, fever, rare infection. |
| Laparoscopic splenectomy | Remove the spleen entirely. | 9095% achieve durable platelet rise. | Bleeding, infection, increased infection risk longterm. |
| Transjugular intrahepatic portosystemic shunt (TIPS) | Lowers portal pressure, indirectly reducing splenic sequestration. | Modest platelet rise in ~30%. | Encephalopathy, shunt dysfunction. |
Choosing between PSE and splenectomy often depends on your overall liver function. For those with a high ChildPugh score (C) or severe portal hypertension, surgeons may shy away from a full splenectomy because the operative risk is steep.
Lifestyle & natural strategies
While meds and procedures do the heavy lifting, some everyday habits can give you a gentle nudge upward:
- Nutrition: Foods rich in vitaminK (leafy greens), folate (beans, lentils), and iron (red meat, fortified cereals) support bonemarrow health.
- Alcohol abstinence: Even moderate drinking can suppress platelet production; cutting it out often leads to a modest rise within weeks.
- Exercise: Light to moderate aerobic activity may shrink spleen size slightly, especially when paired with weight management.
- Stress reduction: Chronic stress can affect hormone balances that indirectly influence platelet counts.
These natural tweaks are great adjuncts, but theyre not a substitute for proven medical therapy when your count is dangerously low. For example, if you have symptoms related to portal hypertension contributing to splenic enlargement, reviewing Portal hypertension symptoms alongside your platelet strategy can help tailor the right approach.
Balancing Benefits & Risks
Every treatment comes with a tradeoff. Lets break down the main considerations so you can have an informed chat with your doctor.
| Option | Benefits | Risks/Sideeffects |
|---|---|---|
| Avatrombopag / Lusutrombopag | Oral, quick rise, avoids transfusion; good for elective procedures. | Potential thromboembolism, liver enzyme elevations, cost. |
| Platelet transfusion | Immediate boostcritical for active bleeding or emergency surgery. | Alloimmunization, shortduration effect (23 days), fluid overload. |
| Partial splenic embolisation | Minimally invasive, durable rise, avoids full organ removal. | Pain, fever, rare infection; not suitable if splenic artery is unsuitable. |
| Laparoscopic splenectomy | Highest platelet increase, longterm effect. | Surgical risks, higher infection susceptibility postop. |
So, how do you decide? Imagine a simple flowchart: if your platelet count is <50K/L and you have an urgent procedure, a transfusion is the fastest route. If you have time (a week or more) before a planned surgery, a TPORA is usually preferred. When counts stay low despite meds, talk to an interventional radiologist about PSE, especially if you want to avoid major surgery.
After any intervention, regular followup labs (often weekly for the first month, then monthly) help catch rebound thrombocytosisa rare but possible overcorrection.
Future Directions
The field isnt standing still. Here are a couple of exciting avenues that could reshape how we manage thrombocytopenia in liver disease:
- New oral TPOmimetics: PhaseII trials in 2025 are showing even higher platelet responses with fewer sideeffects. Expect FDA reviews within the next couple of years.
- Geneediting approaches: Early animal studies suggest that editing liver cells to overproduce thrombopoietin could be a gamechanger, though ethical and safety hurdles remain.
- Artificial spleen devices: Prototype devices aim to filter blood without trapping plateletsstill experimental, but a fascinating concept.
- Telemonitoring platforms: Apps that sync with homebased lab services let patients track platelet trends in real time, making dose adjustments of TPORAs more precise.
All of these are investigational, so for now the best futureproof strategy is to stay informed and keep an open line with your care team.
Conclusion
Low platelets are a common, multifactorial problem in liver disease, but today we have medicines, minimallyinvasive procedures, and lifestyle tweaks that can safely raise counts. The key is to match the strategy to your individual risk profile, the severity of your liver condition, and any upcoming medical proceduresalways in partnership with a hepatologytrained clinician.
As research unfolds, newer oral agents and novel technologies promise even smoother journeys ahead. Until then, you have a solid toolbox to tackle thrombocytopenia headon.
Got a story about how youve managed low platelets, or a question about a specific treatment? Feel free to reach outyour experience could help someone else navigate this tricky terrain.
FAQs
What causes thrombocytopenia in liver disease?
Thrombocytopenia in liver disease is mainly caused by reduced thrombopoietin production and splenic sequestration due to portal hypertension.
How is thrombocytopenia treated in liver disease?
Treatment includes platelet transfusions, thrombopoietin receptor agonists, and sometimes splenic procedures like embolization or splenectomy.
Are thrombopoietin receptor agonists safe for liver disease?
Yes, drugs like avatrombopag and lusutrombopag are FDA-approved and generally safe for raising platelets in liver disease patients.
When is a platelet transfusion needed for liver disease?
A platelet transfusion is used for severe bleeding or before urgent procedures when platelet counts are very low.
Can lifestyle changes help with thrombocytopenia in liver disease?
Lifestyle changes like alcohol abstinence and good nutrition support platelet health but are not substitutes for medical treatment.