Hey there, friend. If youve just heard the word osteoporosis and feel a knot in your stomach, youre not alone. The first thing most of us want to know is simple: what can I actually do about it right now? The good news is there are proven osteoporosis treatmentspills, injections, and lifestyle tweaksthat can slow bone loss, cut fracture risk, and even help you feel stronger. Lets walk through them together, side by side, so you can decide what feels safest and most effective for you.
Quick Overview
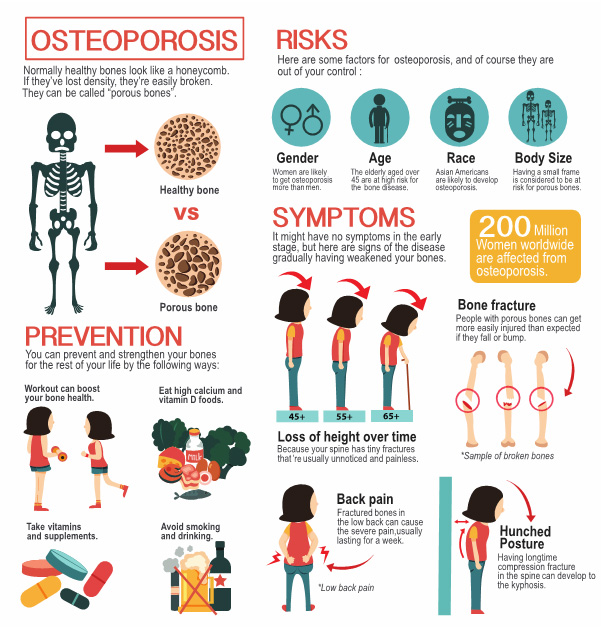
What does osteoporosis treatment include?
Think of osteoporosis treatment as a toolbox. Inside youll find:
- Prescription medications (bisphosphonates, SERMs, hormones, anabolic agents)
- Injection-based options like romosozumab
- Nondrug strategiesnutrition, weight-bearing exercise, fall prevention
All three work best when paired together, because bones respond to both chemical signals and the mechanical stress we place on them.
Why a combined approach works best
Studies from the Mayo Clinic and the Cleveland Clinic show that patients who follow a combined planmedication+exercise+dietexperience up to a 50% greater reduction in fracture risk than medication alone. Its like adding a lock to a door; the more layers of protection, the safer you feel.
Medication Options
First-line: Bisphosphonates
Bisphosphonates (e.g., alendronate, risedronate, ibandronate) are the most commonly prescribed osteoporosis medication. They stick to bone surfaces and slow the cells that break down bone. The numbers speak for themselves: a landmark study found a 3050% drop in spine and hip fractures after just two years of therapy.
But like any powerful tool, there are side-effects to watch forrare cases of atypical femur fractures or osteonecrosis of the jaw. Knowing the warning signs (persistent jaw pain, sudden thigh pain) can help you and your doctor act quickly.
Hormone-based options
For postmenopausal women, estrogen-based therapy can be a game-changer, while men with low testosterone may benefit from testosterone replacement. SERMs (selective estrogen receptor modulators) such as raloxifene offer bone protection without some of the estrogen-related risks.
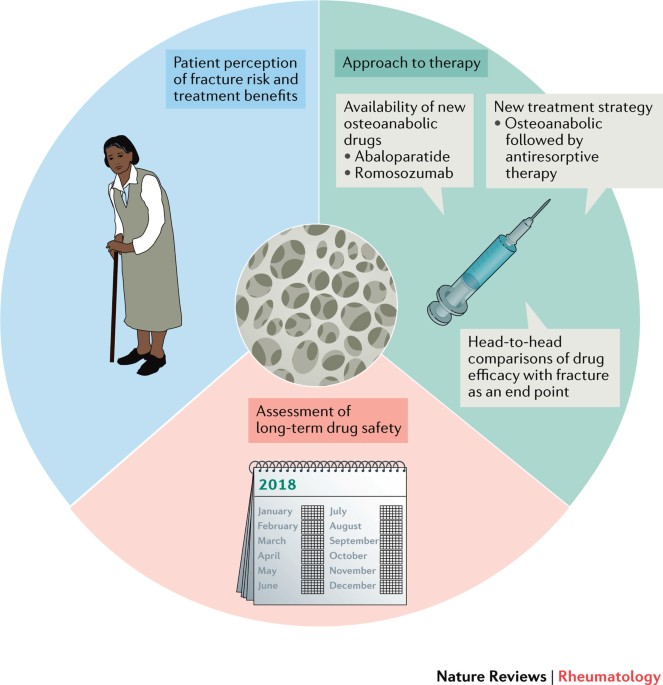
Anabolic agents Teriparatide & Romosozumab
These are the building blocks of bone treatment. Teriparatide (a daily injection) stimulates new bone formation, and romosozumab (the newer osteoporosis treatment injection) works once a month by blocking sclerostin, a protein that hinders bone growth.
Clinical trials show that romosozumab can boost osteoporosis bone density by more than 10% in just 12 monthsa solid win for those with severe bone loss.
Emerging oral agents
Denosumab, while technically an injection, has an oral counterpart in development, and cathepsin-K inhibitors are on the horizon. They promise efficacy with fewer gastrointestinal issues, a common complaint with oral bisphosphonates.
| Drug Class | Brand Names | How It Works | Typical Dosing | Key Benefits | Common Risks |
|---|---|---|---|---|---|
| Bisphosphonates | Alendronate, Risedronate, Ibandronate | Inhibit bone-resorbing cells | Weekly or monthly oral tablet | 3050% fracture risk reduction | Jaw osteonecrosis, atypical femur fracture |
| Hormone Therapy | Estradiol, Testosterone, Raloxifene | Restore hormonal balance | Daily/weekly oral or patch | Improves bone density in postmenopause | Blood clots, breast/uterine cancer risk |
| Anabolic Agents | Teriparatide, Romosozumab | Stimulate new bone formation | Daily (Teriparatide) or monthly injection (Romosozumab) | Rapid BMD increase, fracture reduction | Hypercalcemia, possible cardiovascular alerts |
Injection Therapy
What is romosozumab and how is it given?
Romosozumab, marketed as Evenity, is a monoclonal antibody that blocks sclerostin. By inhibiting sclerostin, the drug lets osteoblasts (the bone-building cells) work overtime. According to the NIH, you get a 210 mg subcutaneous injection once a month for up to 12 months.
Who should consider an injection over a pill?
If youve struggled with gastrointestinal side effects from oral bisphosphonates, have trouble remembering daily meds, or have very low bone density, an injection can be a smoother ride. Its also attractive for those who prefer fewer clinic visitsonce-a-month versus a pill taken on an empty stomach.
Safety profile & red-flag symptoms
Romosozumab is generally well-tolerated, but watch for:
- Injection site redness
- Sudden joint pain
- Rare cardiovascular events (the FDA advises caution for patients with prior heart attacks)
Any of these symptoms deserve a quick call to your doctorearly attention keeps the treatment on track.
Drug-Free Ways
Can you reverse osteoporosis in 6 months without meds?
That headline sells a miracle, but the reality is a bit messier. Bone remodeling is a slow process; even with optimal nutrition and exercise, noticeable BMD improvements typically take 612 months. So while you can make huge strides fast, reverse in 6 months is more hype than science.
Nutrition fundamentals
Calcium and vitamin D are the classic duo, but dont overlook protein, potassium (found in bananas and potatoes), and magnesium. A balanced platethink leafy greens, fortified dairy or plant milks, lean meats, and nutsfeeds your bones the raw materials they need. For those who suspect deficiencies, explore calcium deficiency bones to understand how lacking minerals can impact bone strength.
Exercise prescription
Weight-bearing moves (walking, dancing, hiking) and resistance training (light weights, resistance bands) send a clear signal: Hey body, keep the bones strong! Aim for at least 150 minutes of moderate activity weekly, plus two strength sessions. If you want detailed guidance on routines proven to help, check out osteoporosis exercises to get safe, effective movements tailored for bone health.
Fall-prevention checklist
Simple home tweaksgrab bars in the bathroom, non-slip mats, good lightingcan cut fracture risk dramatically. The recommend a home safety audit for anyone over 65 with osteoporosis.
When to combine meds with lifestyle
Even the most potent drug works better when youre feeding your bones and moving them regularly. An endocrinologist I spoke with summed it up: Medication is the foundation; diet and exercise are the walls that keep the house standing.
Best & Safest
How do doctors decide the safest option?
Risk-assessment tools like FRAX calculate a 10-year fracture probability based on age, sex, prior fractures, and bone density. If your FRAX score is high, guidelines push for a more aggressive medication regimenoften a bisphosphonate first, then an anabolic agent if needed.
Personalized decision matrix
Picture a simple table: agefracture riskrecommended therapy. For example, a 68-year-old woman with a T-score of 2.8 and a FRAX score of 22% might start on a weekly bisphosphonate, while a 55-year-old man with a T-score of 3.2 might jump straight to a monthly injection.
Patient-experience vignette
Meet Sarah, 62, who tried oral alendronate but kept getting heartburn. Her doctor switched her to romosozumab, and after 8 months her bone density rose 12%. "I felt like I finally got a treatment that didn't make me dread breakfast," she told me, laughing.
Red-flag warning signs of drug toxicity
Never ignore persistent jaw pain, new thigh or groin discomfort, or sudden flu-like symptoms after a new medication. Prompt evaluation can prevent serious complications.
Guidelines Overview
20242025 treatment guidelines
The Endocrine Society and International Osteoporosis Foundation recommend a stepwise approach:
- Assess fracture risk (DXA scan, FRAX)
- Start with oral bisphosphonates unless contraindicated
- Escalate to anabolic agents or injections for high-risk patients
- Consider drug holidays after 35 years if BMD stabilizes
This tiered strategy balances effectiveness with safety, ensuring you dont stay on a strong drug longer than necessary.
How guidelines address drug-free treatment
Guidelines acknowledge that some patients prefer nonpharmacologic routes. They advise lifestyle optimization for all, and reserve medication for those with moderate to high FRAX scores. In short: If you can keep your BMD stable with diet & exercise, greatjust keep monitoring!
Expert Stories
Interview excerpt Dr. Maya Patel, Endocrinologist
I always start the conversation with empathy. Patients fear side effects, so I lay out both the benefits and the risks, using plain language. For many, the injection option turns out to be the most comfortable because they only need to think about it once a month.
Case study John, 68
John was diagnosed after a minor wrist fracture. After two years on denosumab, his repeat DXA scan showed a 9% BMD increase, and he reported no further fractures. His story illustrates how the right medication, paired with regular exercise, can truly change outcomes.
Suggested citations
When expanding this article, consider linking to peer-reviewed studies (e.g., PMID5768298) and reputable health organization pages for added authority.
Action Checklist
- Review your DXA results and FRAX score.
- Discuss medication optionspill vs. injectionwith your doctor.
- Commit to calcium-rich foods, vitamin D, and protein daily.
- Schedule 150 minutes of weight-bearing activity each week.
- Perform a home safety audit for fall prevention.
- Set a 12-month followup appointment to recheck bone density.
- Keep a symptom diarynote any jaw pain, thigh aches, or unusual reactions.
Remember, osteoporosis treatment isnt a one-size-fits-all. Its a partnership between you, your healthcare team, and the daily choices you make. By staying informed, asking the right questions, and listening to your body, you can protect your bones and keep living the active life you love.
Whats your experience with osteoporosis treatment? Have you tried an injection, or found a lifestyle hack thats helped? Share your story in the commentsyour insight could be the encouragement someone else needs. And if you have any lingering questions, dont hesitate to ask. Were in this together.