Got a swollen, painful joint and wondering whether its an infection or a reaction to something that happened earlier? The short answer is: septic arthritis means live germs have invaded the joint, while reactive arthritis is the bodys immunesystem response after an infection elsewhere. Knowing which one youre dealing with can mean the difference between a quickacting IV antibiotic regimen and a course of antiinflammatories, and it can save your joint from permanent damage.
In the next few minutes well walk through exactly what each condition looks like, how doctors tell them apart, and what you can expect if you ever face one of them. Grab a cup of tea, settle in, and lets untangle these two tricky arthritic cousins together.
What Is Septic Arthritis
Definition and Pathophysiology
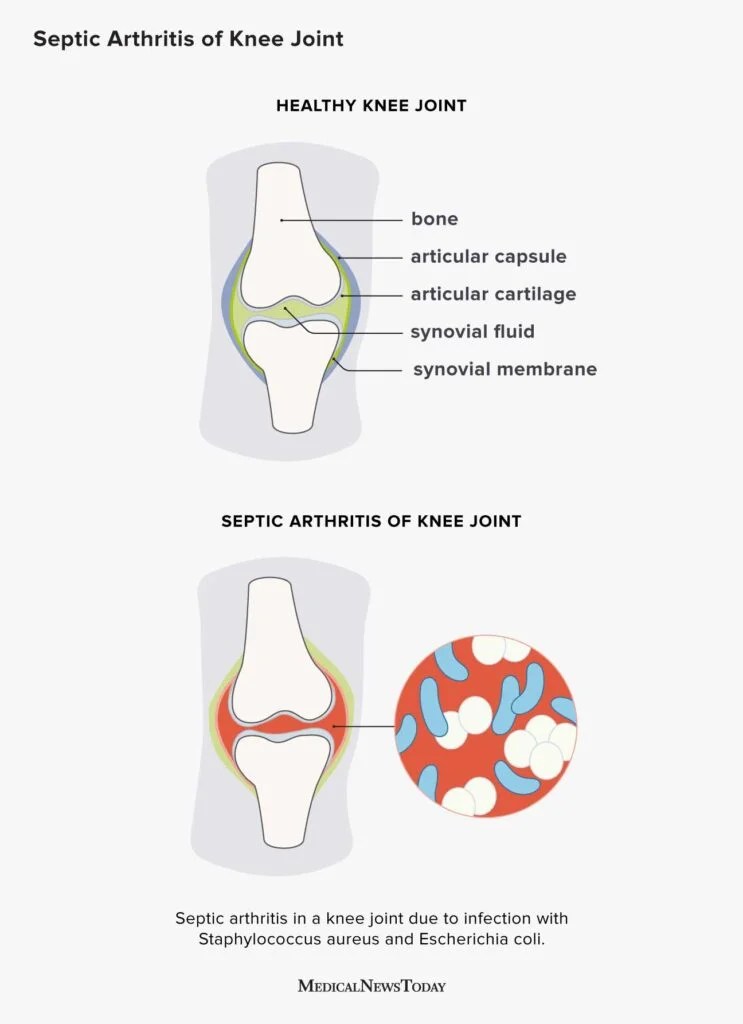
Septic arthritis is an infection inside the joint space. Bacteria, fungi, or rarely viruses slip into the synovial fluid, sparking a rapid inflammatory cascade that can quickly destroy cartilage if left untreated. Think of the joint as a tiny, wellguarded roomonce the invaders break in, the immune system floods the area, and the resulting battle can be brutal.
Causes of Septic Arthritis
Most cases stem from like Staphylococcus aureus (the classic troublemaker), Streptococcus species, and Neisseria gonorrhoeae in sexually active adults. Less common offenders include Gramnegative rods from the gut, fungal organisms in immunocompromised patients, and even mycobacteria in rare settings.
Symptoms and RedFlag Signs
Septic arthritis loves to make a scene: sudden, intense joint pain; swelling that feels warm to the touch; fever; chills; and an overall sense of Im really sick. The knee and hip are frequent targets, but any joint can be hijacked. If you notice a joint thats painful within hours of a fever, its a red flag worth a trip to the ER.
Who Is at Risk?
Children under five, older adults, people with diabetes or rheumatoid arthritis, intravenous drug users, and anyone whos had recent joint surgery or injections are on higher risk. The immune systems guardrails are a bit weaker in these groups, letting germs slip through more easily.
What Is Reactive Arthritis
Definition and Mechanism
Reactive arthritis isnt an infection of the joint itself. Instead, its an immunemediated inflammation that shows up after an infection elsewhereoften in the gastrointestinal or genitourinary tract. The bodys defenders get confused and start attacking the joint lining, even though the joint is technically sterile.
Common Triggers
Typical triggers include Campylobacter, Salmonella, Shigella, and Yersinia from contaminated food, as well as Chlamydia trachomatis from sexually transmitted infections. When these bugs pass through, they leave a molecular fingerprint that can mislead the immune system for weeks afterward.
Triad and Symptoms
The classic reactive arthritis triad consists of arthritis, conjunctivitis (red, itchy eyes), and urethritis (painful urination). Not everyone gets all three, but many will notice at least two. Joint pain often hits the knees, ankles, or feet, and it usually appears 14 weeks after the original infection. The joint fluid is sterilemeaning cultures come back negativewhich is a big clue for clinicians.
Risk Factors
Being HLA-B27 positive dramatically ups the odds, as does being in the 2040 year old age bracket. A prior infection with any of the culprits listed above can set the stage, but the condition is still relatively uncommon overall.
Direct Comparison Table
| Feature | Septic Arthritis | Reactive Arthritis |
|---|---|---|
| Cause | Live pathogen in the joint | Immune response after remote infection |
| Jointfluid culture | Usually positive | Sterile (negative) |
| Onset | Hoursdays | 14 weeks postinfection |
| Systemic signs | Fever, chills, high WBC | Mild fever, possible eye/urinary symptoms |
| Typical joints | Large joints (knee, hip) | Lowerextremity joints, sacroiliac |
| Treatment urgency | Orthopaedic emergency | Outpatient, NSAIDs antibiotics |
| Prognosis | Risk of permanent damage if delayed | Usually selflimiting; |
How Clinicians Differentiate
When a patient walks in with an acutely swollen joint, doctors start with a quick history (any recent infections? fever?), then they tap the joint to draw fluid. If the fluid looks turbid and cultures grow bacteria, its septic arthritis. If the fluid is clear and the patient mentions a recent bout of food poisoning or a urinary infection, reactive arthritis climbs higher on the differential. In USMLEstyle questions, look for joint aspiration yields purulent fluid for septic arthritis, and negative cultures + eye or urethral symptoms for reactive arthritis.
Diagnostic Checklist
- Complete blood count (CBC) elevated white cells in septic cases.
- ESR/CRP both can be raised, but higher spikes often point to infection.
- Joint aspiration gram stain, culture, and crystal analysis.
- PCR for Chlamydia if GU source suspected.
- HLAB27 testing helpful for confirming reactive arthritis risk.
- Imaging plain Xray may be normal early; MRI can reveal early bone involvement, useful when considering .
Treatment Strategies
Septic Arthritis Management
Time is cartilage. The standard approach is urgent joint drainageeither needle aspiration, arthroscopy, or open surgerycombined with empiric IV antibiotics (often vancomycin plus ceftriaxone) while awaiting culture results. Once the pathogen is identified, antibiotics are narrowed and continued for 34 weeks, sometimes longer if bone involvement (osteomyelitis) is present.
Reactive Arthritis Management
Since theres no infection inside the joint, treatment focuses on calming the immune system. Firstline therapy is NSAIDs (ibuprofen, naproxen) to ease pain and swelling. If symptoms persist beyond a few weeks, a short course of corticosteroidseither oral or intraarticularcan provide relief. For chronic or severe cases, diseasemodifying agents like sulfasalazine or methotrexate may be considered. Dont forget the underlying trigger: a single dose of azithromycin can clear a lingering Chlamydia infection, and treating the gut infection (often with hydration and possibly antibiotics) helps stop the immune cascade.
Rehabilitation and Followup
Both conditions benefit from early physiotherapy once acute inflammation eases. Gentle rangeofmotion exercises prevent stiffness, while strength training restores confidence in the joint. Regular followup appointments let doctors monitor inflammatory markers and adjust antibiotics or antiinflammatories as needed. In septic arthritis, a repeat joint aspiration may be required to ensure the infection is truly gone.
RealWorld Cases and Pearls
Case A Septic Arthritis in a Child
Emily, a sevenyearold, woke up with a hot, swollen knee that wouldnt let her walk to school. Her parents noticed a fever of 101F. In the ER, arthrocentesis revealed purulent fluid; cultures grew Staphylococcus aureus. She underwent urgent arthroscopic washout and a twoweek course of IV cefazolin, followed by oral antibiotics. Six weeks later, her knee was painfree and fully functionala reminder that swift action saves joints.
Case B Reactive Arthritis After Food Poisoning
Jake, 28, enjoyed a weekend road trip that ended with a bout of severe diarrhea from undercooked chicken. Two weeks later, his left ankle swelled, his eyes turned red, and he felt a burning sensation when he urinated. Tests for joint infection were negative, but a urine PCR was positive for Chlamydia. He started a short course of NSAIDs, received azithromycin for the hidden infection, and was advised to rest the ankle. Within three months, his symptoms faded, and hes back to hiking.
Clinical Pearls
- If joint fluid is purulent, treat as septic arthritis until proven otherwise.
- Reactive arthritis often presents with extraarticular signseyes and urinary tract.
- HLAB27 positivity doesnt guarantee disease, but it raises suspicion.
- Never overlook osteomyelitis when septic arthritis involves a boneadjacent joint.
- Patient education is key: early presentation can prevent irreversible damage.
Bottom Line
Septic arthritis and reactive arthritis may sound similar, but theyre fundamentally different beastsone is a true infection that demands immediate drainage and antibiotics, the other is an immunedriven flare after an infection elsewhere, usually managed with antiinflammatories and treatment of the original trigger. Recognizing the redflag signs, getting the right labs, and acting promptly can protect your joints and your quality of life.
If youve ever dealt with a swollen joint, or if a friend tells you theyre just having arthritis, remember: the cause matters. Talk to a healthcare professional, especially if you have fever, rapid swelling, or newonset eye or urinary symptoms. And feel free to share your own story or ask questions in the commentsyour experience could help someone else navigate the same confusing crossroads.
FAQs
What is the main difference between septic arthritis and reactive arthritis?
Septic arthritis is caused by a live infection inside the joint, whereas reactive arthritis is an immune reaction that occurs after an infection elsewhere in the body but with no live germs in the joint itself.
How can doctors tell septic arthritis apart from reactive arthritis?
Doctors differentiate by joint fluid analysis: septic arthritis usually shows purulent fluid with positive cultures for bacteria, while reactive arthritis joint fluid is sterile with negative cultures.
Which joints are commonly affected in septic arthritis and reactive arthritis?
Septic arthritis typically affects large joints like the knee and hip, while reactive arthritis often involves lower extremity joints such as knees, ankles, feet, and sacroiliac joints.
What are the typical symptoms of septic arthritis compared to reactive arthritis?
Septic arthritis presents with sudden severe joint pain, swelling, fever, and chills. Reactive arthritis usually appears 1-4 weeks after an infection and can include joint pain, eye inflammation, and urinary symptoms, often with milder systemic signs.
What treatments are used for septic arthritis and reactive arthritis?
Septic arthritis requires urgent joint drainage and intravenous antibiotics. Reactive arthritis is treated with anti-inflammatory medications like NSAIDs, corticosteroids, and addressing the triggering infection if present.