Quick Answer Snapshot
In plain terms, modern TAVR gives a 5year survival of roughly 6575% for low and intermediaterisk patients, while the 30day death risk has dropped to under0.5%. Those numbers are very close to, or even a little better than, what youd expect from an agematched healthy population. In short, if youre weighing TAVR against surgery, the odds are looking increasingly favorable.
How Success Is Measured
What success rate really means
When cardiologists talk about the tavr success rate, theyre really juggling a handful of metrics:
- Procedural success the valve is placed without major issues.
- Shortterm outcomes 30day mortality, stroke, need for a permanent pacemaker.
- Longterm outcomes survival at 1, 3, and 5years, plus valve durability.
Benchmark numbers from 20232025 studies
Heres a quick snapshot of the most recent data (20232024) pulled from large registries and peerreviewed trials:
- 30day mortality: 0.30.5% in highvolume centers ().
- 5year survival: 6475% for lowrisk patients, compared with about 81% for the same age group without heart disease ().
- Allcause 5year mortality across all risk groups: 45.8% (mean followup 5.4years) ().
Suggested visual aid
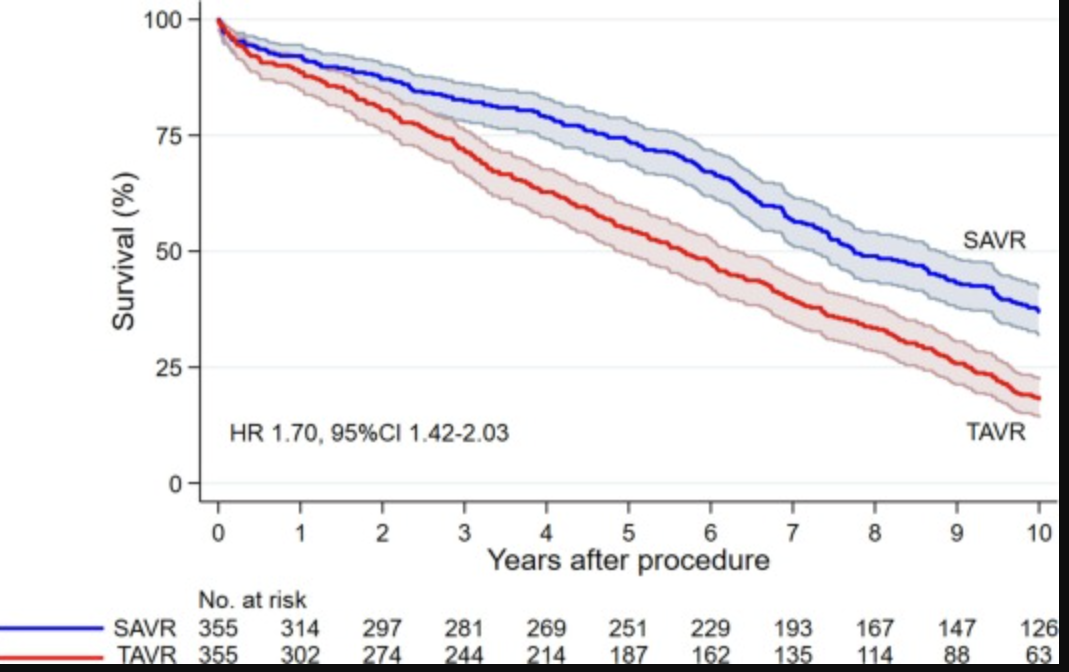
| Metric | TAVR | SAVR |
|---|---|---|
| 30day mortality | 0.4% | 0.2% |
| 1yr survival | 88% | 91% |
| 3yr survival | 75% | 80% |
| 5yr survival | 68% | 78% |
Who Benefits Most
Lowrisk vs. intermediaterisk vs. highrisk patients
The European System for Cardiac Operative Risk Evaluation (EuroSCORE) and the Society of Thoracic Surgeons (STS) score split patients into low, intermediate, and high risk. In lowrisk cohorts, 5year survival hovers around 70%, while highrisk groups see a bit lessstill respectable given how sick they were before the procedure.
TAVR success rate in the elderly
If youre 80 or older, the numbers shift slightly. Studies show a 5year survival of about 60% for octogenarians, compared with 70% in younger groups. Stroke risk nudges upward (2% at 30days) and the chance of needing a pacemaker creeps up a touch, but the procedures minimally invasive nature still means faster recovery and less time in the ICU.
Younger patients and the longest living story
It used to be thought that only seniors needed TAVR, but now highlighted a 58yearold whos now 12years postTAVR and living a full, active life. Thats the longestliving TAVR patient documented so far, and it shows the technology is maturing fast enough for younger folks to consider it seriously.
Realworld anecdote
John, a 68yearold retired teacher, was flagged as lowrisk in 2022. He chose TAVR, had a smooth procedure, and at his 5year checkup hes still hiking, gardening, and refusing to use a walker. Stories like Johns remind us that behind every statistic is a person who gets a second wind.
Risks & Complications Overview
Major complications to watch
Even the bestrated treatments have downsides. Heres what the data say:
- Stroke: roughly 2% at 30days.
- Permanent pacemaker: dropped from 25% a decade ago to about 10% with newer devices ().
- Vascular injury or bleeding: 35%.
- Acute kidney injury: 12%.
Death during TAVR procedure
Early trials reported procedural mortality rates of 58%, but thanks to better imaging, refined catheters, and seasoned heart teams, todays inprocedure death rate is under 0.1% at highvolume centers. Its a testament to how quickly the field has evolved.
Comparing TAVR vs. SAVR in the 2024 guidelines
The 2024 ACC/AHA guideline update states that for low and intermediaterisk patients, TAVR is a ClassI recommendationmeaning its considered a standard of careprovided the center performs more than 100 procedures a year. For highrisk patients, both TAVR and SAVR remain viable, with the choice driven by anatomy, comorbidities, and patient preference.
Sidebar: CenterVolume Effect
One study out of Duke showed that hospitals doing over 100 TAVR cases annually cut 30day mortality by about 30% compared with lowvolume sites. If youre shopping for a team, ask them how many TAVR procedures theyve done in the past yearthat simple question can make a big difference.
LongTerm Outlook Overview
10year life expectancy after TAVR
Data beyond eight years are still limited, but extrapolations suggest that roughly half of lowrisk patients survive ten years postprocedure. The newest generation of valves show structural deterioration rates of less than 2% per year after the fiveyear mark, which is encouraging for anyone hoping for a decadeplus horizon.
Valve durability and reintervention
Most modern bioprosthetic valves maintain good function for at least 1012 years. When they do start to wear, the emerging TAVRinTAVR techniqueplacing a second transcatheter valve inside the firsthas shown promising early results, making repeat procedures less daunting.
Practical tip for patients
Stay on top of your followup schedule: a yearly echocardiogram, a symptom diary, and a hearthealthy lifestyle (lowsalt diet, regular walks, and blood pressure checks). Small habits add up, and they help you and your heart team spot trouble before it becomes serious.
Making Your Decision
Questions to ask your heart team
- What is my STS risk score and how does it translate to expected survival?
- How many TAVR procedures does this center perform each year?
- What are the specific risks for someone my age and with my anatomy?
- If the valve were to fail, what are the reintervention options?
Balancing benefits vs. risks
Think of it like weighing two sides of a scale. On one side you have quick recovery, less pain, and a lower earlymortality chance. On the other side, you have potential need for a pacemaker, slightly lower longterm survival, and the unknowns of valve durability. A simple prosandcons table can clarify the picture:
| Pros | Cons |
|---|---|
| Minimal incision, shorter hospital stay | ~2% stroke risk |
| 30day mortality under 0.5% | Potential pacemaker requirement |
| Suitable for highrisk or frail patients | Longterm durability still under study |
When SAVR might still be better
If you have a bicuspid aortic valve, extreme calcium buildup, or youre under 55 and expect to live many more decades, surgical aortic valve replacement (SAVR) can still be the gold standard. The 2024 guidelines highlight those scenarios as the main reasons to lean toward surgery.
Key Takeaways Summary
Modern TAVR delivers a solid success rateroughly twothirds of patients alive at five yearsand early mortality has plummeted to under half a percent in experienced centers. Age, overall health, and the procedure volume of the chosen hospital are the biggest drivers of your outcome. While complications like stroke or a pacemaker remain possible, theyre relatively rare and often manageable. Ultimately, the best decision comes from a transparent conversation with a boardcertified interventional cardiologist who can translate the numbers into what they mean for your life.
For patients concerned about swelling or fluid buildup after valve procedurescommon issues in heart failuretalking with your care team about heart failure edema treatment options can be helpful for managing symptoms during recovery.
Whats your take on the data? Have you or a loved one faced the TAVR vs. SAVR crossroads? Share your story in the comments, or reach out if you have questionslets navigate this together.
FAQs
What is the current 30‑day mortality rate for TAVR?
In high‑volume centers the 30‑day mortality for TAVR has fallen to roughly 0.3‑0.5 %.
How does TAVR survival compare to surgical valve replacement at 5 years?
Recent registries show a 5‑year survival of about 68 % after TAVR versus roughly 78 % after surgical aortic valve replacement.
Who are the best candidates for TAVR?
Low‑ and intermediate‑risk patients, especially those aged 70 +, frail individuals, and patients with comorbidities that make open surgery risky are the typical beneficiaries.
What are the most common complications after TAVR?
The major complications reported in 2024 studies are stroke (~2 % at 30 days), need for a permanent pacemaker (~10 %), vascular injury or bleeding (3‑5 %), and acute kidney injury (1‑2 %).
Can a TAVR valve be replaced if it fails?
Yes. The “TAVR‑in‑TAVR” approach—implanting a second transcatheter valve inside the first—is increasingly used when the initial valve shows structural deterioration.