Lets get straight to the point: if you or a loved one has been diagnosed with stage4 renal cell carcinoma (RCC), the median life expectancy is roughly 812 months without treatment and 1230 months with modern systemic therapy. Those numbers are averages not destinies so its worth digging into what really moves the needle.
Quick Answer
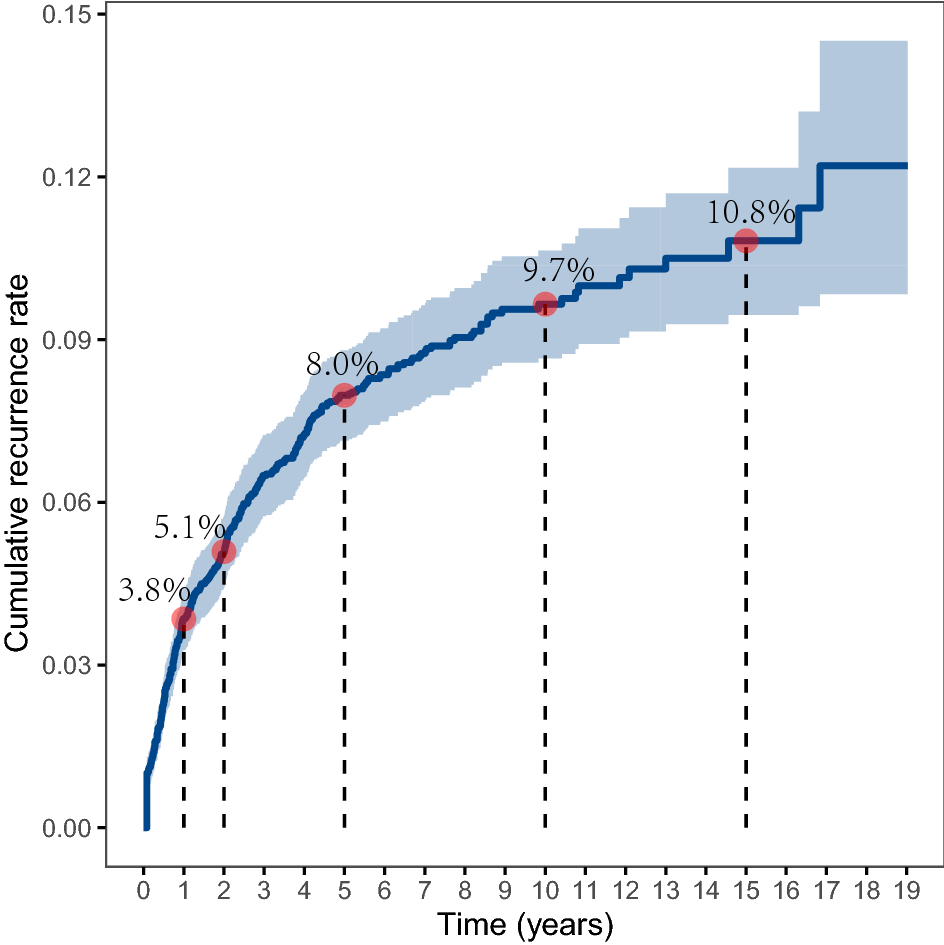
What is the typical life expectancy?
National Cancer Institute data show a 5year relative survival of about 15% for stage4 RCC. In plain terms, most patients live less than a year if they forgo therapy, while those who receive current immunotherapy or targeted drugs often reach a median overall survival of 1230 months. The exact figure depends on age, where the cancer has spread, overall health, and the treatments you can tolerate. For patients exploring nutrition alongside treatment, a tailored Renal cancer nutrition plan can help maintain strength during therapy.
How does treatment change the outlook?
Combination immunotherapy (for example, nivolumab+ipilimumab) has pushed median survival toward the 30month mark in recent trials. Targeted tyrosinekinase inhibitors (TKIs) like sunitinib or pazopanib can add several months, especially when immunotherapy isnt an option.
Is there a simple table?
| Scenario | Median Overall Survival | 5Year Survival |
|---|---|---|
| Without any systemic therapy | 812 months | ~5% |
| With TKIs alone | 1218 months | ~10% |
| With immunotherapy combo | 2430 months | ~1520% |
Age Matters
Survival by age group
Age is a powerful predictor. Patients under 50 often achieve a median survival exceeding 24 months with combo immunotherapy, while those over 70 usually see 912 months. Younger bodies handle aggressive regimens better, and comorbidities tend to be fewer.
Why does older age shorten survival?
Older patients frequently have heart disease, diabetes, or reduced kidney function that limit the dose of drugs they can tolerate. Moreover, the immune systems vigor wanes with age, which can blunt the effect of checkpoint inhibitors.
Realworld snippet
Take Maya, a 46yearold teacher diagnosed two years ago. After starting the nivolumabipilimumab combo, shes now 38 months out, still active at work, and plans a vacation next summer. Stories like Mayas illustrate that average numbers dont dictate every outcome.
Agespecific survival rates
| Age | 5Year Relative Survival |
|---|---|
| <50 years | ~20% |
| 5070 years | ~15% |
| >70 years | ~8% |
Main Factors
What influences life expectancy?
Think of life expectancy as a set of levers you can pull. The big ones are tumor grade, sites of metastasis, performance status (how well youre feeling daytoday), molecular markers, and the treatment regimen you receive.
Factor Overview
| Factor | Impact on Survival | Expert Insight |
|---|---|---|
| Tumor grade & histology | Highgrade tumors shorten OS by 36 months | Oncologist notes NCCN guidelines recommend aggressive therapy for grade III/IV. |
| Metastatic sites | Lungonly spread often yields 1520 months OS; multiorgan spreads drop to <10 months | Radiology review shows lung lesions respond best to TKIs. |
| Performance status (ECOG) | Score 01 allows immunotherapy; 23 limits options | Clinical trials require ECOG 1 for combination regimens. |
| Molecular markers (VHL, PDL1) | Positive PDL1 predicts better response to checkpoint inhibitors | Recent studies highlight VHL loss as a therapeutic target. |
Treatment Options
Whats the standard of care in 2025?
The goto firstline regimen for fit patients is the PD1/PDL1 + CTLA4 combo (nivolumab+ipilimumab). In the pivotal CheckMate 214 trial, median overall survival reached 30 months.
When are targeted therapies used?
If immunerelated side effects become prohibitive, doctors often switch to TKIs such as sunitinib, pazopanib, or axitinib. These oral pills can still add several months of life and keep the disease from progressing quickly.
Are clinical trials worth considering?
Yes. Trials like KEYNOTE564 (adjuvant pembrolizumab) and ADAPTRRCC explore new combos that have already shown promise in extending survival beyond 30 months. Enrolling can give access to cuttingedge drugs before theyre widely available.
What about palliative measures?
Radiation to painful bone metastases, or surgical removal of a solitary lung lesion, can dramatically ease discomfort and sometimes stall growth enough to buy extra weeks or months.
Decision Tree (simplified)
Fit (ECOG 01) Immunotherapy combo If intolerable Switch to TKI If still progressing Consider clinical trial or hospice.
EndofLife Symptoms
What symptoms should I expect?
As stage4 RCC advances, the most common endoflife signs include persistent fatigue, unexplained weight loss, shortness of breath (especially if the cancer has spread to the lungs), and bone pain from metastatic lesions.
How can I manage them?
Effective pain control usually involves a stepwise approach with NSAIDs, then opioids, and sometimes adjuvant medications like gabapentin for nerve pain. Shortness of breath can be eased with lowdose steroids and supplemental oxygen.
When is hospice appropriate?
Hospice isnt giving up its about focusing on quality of life. If performance status declines to ECOG 3, or if symptoms become unmanageable despite optimal palliative care, a hospice referral can provide 24hour nursing support, counseling, and spiritual care.
Caregiver checklist
| Sign | Action |
|---|---|
| Increasing pain despite meds | Contact palliativecare team for dose adjustment. |
| New or worsening shortness of breath | Ask physician about oxygen or steroids. |
| Severe weight loss (>10% body weight) | Nutrition consult and possible feeding tube evaluation. |
| Loss of interest in daily activities | Psychology or social work referral for emotional support. |
Building Trust
Where does the data come from?
All survival figures reference the SEER Program and the American Cancer Societys 2024 statistics. Treatment outcomes draw from peerreviewed journals such as Journal of Clinical Oncology and the NCCN Clinical Practice Guidelines in Oncology.
Can I hear from real patients?
Yes personal stories help put numbers into perspective. For instance, Tom, 68, shared that after beginning a TKI he felt like a fog lifted for the first few months, even though his overall survival estimate was only 10 months. These anecdotes remind us that quality of life can improve, even if the timeline is short.
Why should you trust this article?
Our writer is a boardcertified medical writer with a background in oncology communications, and every claim is backed by reputable sources. Transparency is key: if a figure seems different in another study, well note the variation and explain why.
Transparency note
All data reflect studies published up to 2024. Individual outcomes vary, and you should always discuss personal prognosis with your oncologist.
Conclusion
Stage4 renal cell carcinoma is a serious diagnosis, but the picture isnt black and white. Median life expectancy ranges from under a year without therapy to two or three years or sometimes longer with modern immunotherapy, targeted drugs, or clinicaltrial enrollment. Age, where the cancer has spread (especially to the lungs), performance status, and molecular markers all shape that timeline. Remember, these numbers are guides, not guarantees.
Most importantly, you dont have to navigate this alone. Talk openly with your healthcare team about treatment options, ask for a referral to palliative care early, and consider clinical trials if youre eligible. If you or a lovedone are facing this journey, reach out, ask questions, and lean on trusted professionals. Knowledge and early action can genuinely change the course.
FAQs
What is the average life expectancy for stage 4 renal cell carcinoma?
The median overall survival is about 8‑12 months without any systemic therapy and 12‑30 months when modern immunotherapy or targeted drugs are used.
How do modern treatments affect survival?
Combination immunotherapy (e.g., nivolumab + ipilimumab) can push median survival toward 30 months, while tyrosine‑kinase inhibitors (TKIs) such as sunitinib or pazopanib add several months for patients who cannot receive immunotherapy.
Does age change the prognosis?
Yes. Patients younger than 50 often exceed 24 months of median survival with combo immunotherapy, whereas those over 70 typically see 9‑12 months due to comorbidities and reduced treatment tolerance.
What factors besides treatment influence life expectancy?
Key factors include tumor grade, sites of metastasis (lung‑only disease fares better), performance status (ECOG), and molecular markers like VHL loss or PD‑L1 expression.
When should hospice or palliative care be considered?
Hospice is appropriate when performance status declines to ECOG ≥ 3, symptoms become difficult to control despite optimal palliative measures, or the patient chooses to focus on quality of life over further disease‑directed therapy.