Understanding the Splenic Flexure
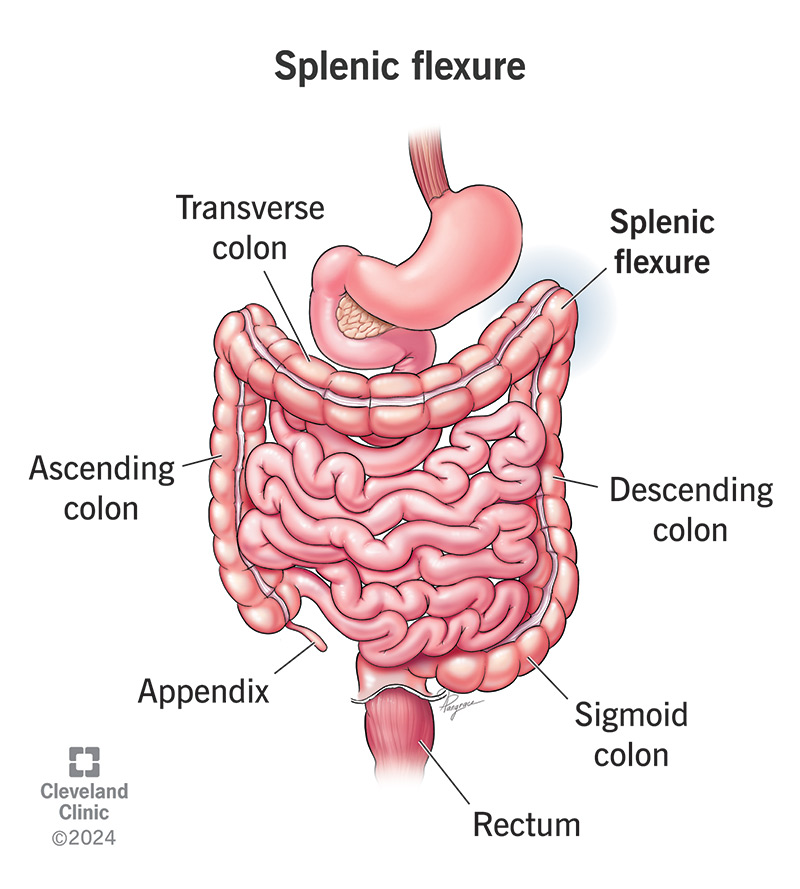
The splenic flexure is the bend where the transverse colon turns down into the descending colon, tucked just under your left rib cage. Think of it as a short, winding road in the colon thats a bit of a bottleneck because of its tight turn and unique blood supply. This watershed area gets blood from two different arteries, making it a spot that can be vulnerable to problems, including cancer.
Why Cancer Happens Here
Most of the time, colorectal cancer develops in the rectum or sigmoid colon, but about 510% of cases pop up at the splenic flexure. Risk factors are much the same as elsewhere in the colon: age over 50, a family history of colorectal cancer, longstanding inflammatory bowel disease, a diet low in fiber and high in red or processed meat, smoking, and excessive alcohol consumption. The same habits that fuel other colon cancers can also set the stage at this bend.
Splenic Flexure Syndrome vs. Cancer
Its easy to confuse splenic flexure cancer with splenic flexure syndrome, a benign condition where trapped gas causes bloating and discomfort. The key difference is that syndromerelated pain usually eases after passing gas or changing position, while cancerrelated pain is persistent, may worsen, and is often accompanied by other redflag symptoms like weight loss or bleeding.
What Experts Say
According to a overview, the splenic flexures location makes early detection tricky, which is why knowing the warning signs matters.
Key Cancer Symptoms
Below is a snapshot of the most common symptoms that should raise a red flag. If you notice any of these persisting for more than a couple of weeks, its worth a chat with your doctor.
| Symptom | Typical Presentation | Why It Happens |
|---|---|---|
| Leftupper abdominal pain | Cramping or sharp pain under the left ribs, may radiate to the back | Tumor pressing on surrounding tissue |
| Change in bowel habits | Constipation, alternating diarrhea, narrower stools | Partial blockage at the flexure |
| Unexplained weight loss | Loss of >5% body weight within 6months | Increased metabolic demand of cancer cells |
| Fatigue & anemia | Pale skin, shortness of breath, feeling rundown | Chronic blood loss or inflammatory response |
| Rectal bleeding or occult blood | Dark stools, positive fecal occult blood test | Ulceration of the tumor |
Spotting the Difference
When you feel uncomfortable after a big meal, think gas. But when the pain lingers, wakes you up at night, or comes with weight loss, its time to take it seriously. The body rarely liespersistent, unexplained symptoms deserve attention.
A RealWorld Tale
Maria, 58, thought her persistent bloating was just a side effect of her new highfiber diet. After three months of just living with it, a routine colonoscopy revealed a 3cm lesion right at her splenic flexure. Early discovery meant a straightforward laparoscopic resection and a much brighter outlook.
How Diagnosis Works
Lets demystify the journey from something feels off to a definitive diagnosis. Understanding each step can calm the nerves and give you a sense of control.
FirstLine Checks
Your doctor will start with a thorough medical history and a physical exam, focusing on any tenderness near the left upper abdomen. Youll likely be asked about family history, diet, and lifestyle.
StoolBased Tests
Noninvasive tests like the fecal immunochemical test (FIT) or guaiacbased fecal occult blood test (gFOBT) can detect hidden blood. Some newer panels also look for DNA markers associated with colorectal cancer. If any of these come back positive, its a cue to move to imaging.
Imaging and Endoscopy
- CT colonography: Offers a detailed view of the colons interior, highlighting masses or thickened walls.
- Colonoscopy: The goldstandard. A flexible camera lets the doctor see the flexure directly and take biopsies if something looks suspicious. If a biopsy confirms cancer, questions about prognosis or colon cancer genetic testing may follow to guide treatment.
- MRI & PET scans: Reserved for stagingdetermining whether the cancer has spread to nearby lymph nodes or distant organs.
Guidelines Worth a Look
The recommend colonoscopy as the definitive diagnostic tool for any abnormal finding on imaging or stool testing.
Staging and Survival Rates
Once a biopsy confirms cancer, doctors assign a stage using the AJCC TNM systemTumor size, Node involvement, and Metastasis. Heres a quick rundown:
- Stage I: Cancer confined to the inner lining 5year survival 90%.
- Stage II: Grows into deeper layers survival drops to about 75%.
- Stage III: Involves regional lymph nodes roughly 55% survival.
- Stage IV: Metastatic disease survival can be under 30%.
These numbers are averages; many factorsage, overall health, response to treatmentshape individual outcomes. Still, catching the disease early dramatically improves the odds.
Treatment Paths Explained
When it comes to beating splenic flexure cancer, a multidisciplinary team usually steps in: surgeons, medical oncologists, radiation oncologists, and nutritionists all play a part. Below is a friendly guide to the most common options.
Surgical Options
The cornerstone of curative treatment is surgeryspecifically a leftside hemicolectomy, where the segment containing the flexure is removed along with nearby lymph nodes. Surgeons can perform the operation either open (traditional incision) or laparoscopic (small keyhole incisions). Laparoscopic surgery generally means less pain, a shorter hospital stay, and a quicker return to daily life.
Adjuvant Therapies
Most patients also receive chemotherapy after surgery to wipe out any microscopic cancer cells that might have slipped away. Common regimens include FOLFOX (folinic acid, fluorouracil, oxaliplatin) or CAPEOX (capecitabine plus oxaliplatin). The exact plan depends on the stage and molecular profile of the tumor.
Targeted & Immunotherapy
If the tumor tests positive for certain genetic alterationslike KRAS, NRAS, or BRAF mutationstargeted drugs can be added to the regimen. For tumors that are microsatellite instabilityhigh (MSIH) or have mismatch repair deficiency (dMMR), checkpoint inhibitors such as pembrolizumab have shown promising results.
Patient Tip
Ask your surgeon about an ERAS (Enhanced Recovery After Surgery) protocol. Its a set of evidencebased stepsearly feeding, mobilization, pain controlthat can shave days off your hospital stay and reduce complications.
NonSurgical Management
In rare cases where surgery isnt feasible (e.g., severe comorbidities), radiation therapy or systemic chemotherapy may be used to control the disease. These approaches are typically palliative, aiming to relieve symptoms and prolong life.
Life After Diagnosis
Getting through treatment is a huge milestone, but the journey doesnt end there. Survivorship care focuses on monitoring, lifestyle, and emotional wellbeing.
FollowUp Schedule
Most oncologists recommend a colonoscopy one year after surgery, then every three years if everything looks clear. Imaging (CT scans) is usually done annually for the first few years to watch for recurrence.
Healthy Living Tips
- Fiberrich diet: Aim for at least 2530g of fiber dailythink whole grains, beans, fruits, and vegetables.
- Regular activity: Even a 30minute walk most days can lower the risk of recurrence.
- Avoid tobacco & limit alcohol: Both are linked to poorer outcomes.
- Weight management: Maintaining a healthy BMI helps reduce inflammation.
Support Networks
Living with a cancer diagnosis can feel isolating. Groups like the Colorectal Cancer Alliance offer peer support, educational webinars, and counseling services. You dont have to walk this road alone.
Story of Resilience
James, 62, finished his treatment a year ago and joined a survivorship program that included gentle yoga and walking clubs. He says the routine not only boosted his stamina but also gave him a community of people who get it.
Bottom Line Take Action Today
Understanding splenic flexure cancer symptoms is the first step toward early detection and better outcomes. Persistent leftupper abdominal pain, unexplained weight loss, changes in bowel habits, fatigue, or any sign of bleeding should never be ignored. Talk openly with your healthcare provider, stick to recommended screening schedules, and adopt a lifestyle that supports colon health.
Remember, knowledge empowers you to act quickly and confidently. If anything in this article resonated with youor sparked a questiondont hesitate to reach out to a medical professional. Your health is worth every ounce of attention.
FAQs
What are the common symptoms of splenic flexure cancer?
Common symptoms include persistent left upper abdominal pain, changes in bowel habits (constipation or diarrhea), unexplained weight loss, fatigue with anemia, and rectal bleeding or positive occult blood in stool.
How can splenic flexure cancer symptoms be distinguished from splenic flexure syndrome?
Splenic flexure syndrome causes gas-related pain that usually eases after passing gas or changing position, while cancer-related pain is persistent, may worsen over time, and is accompanied by other signs like weight loss or bleeding.
Why is early detection of splenic flexure cancer challenging?
The splenic flexure's location under the left rib cage and its anatomical bend make early tumors hard to detect, often causing vague symptoms that can be mistaken for less serious conditions.
What diagnostic tests are used to confirm splenic flexure cancer?
Initial tests include stool-based blood tests like fecal immunochemical tests, followed by imaging such as CT colonography and colonoscopy, which allows direct visualization and biopsy of suspicious lesions.
What lifestyle changes can help after a splenic flexure cancer diagnosis?
A fiber-rich diet, regular physical activity, avoiding tobacco and limiting alcohol, and maintaining a healthy weight are recommended to support recovery and reduce risk of recurrence.