Why the Difference Matters
Understanding whether youre facing septic arthritis or osteomyelitis isnt just academicit can be a matter of life and limb. Septic arthritis can destroy a joint in days and, if left untreated, can lead to sepsis, which can be fatal. Osteomyelitis, on the other hand, tends to linger, sometimes turning into chronic bone infection that compromises growth plates in children or forces surgery in adults. Knowing the difference lets doctors target the right antibiotics, plan the correct surgery, and ultimately protect you from longterm disability.
Clinical Differences Explained
| Feature | Septic Arthritis | Osteomyelitis |
|---|---|---|
| Onset | Sudden, severe joint pain | Gradual bone ache, often weeks |
| Fever | Highgrade, often >101F | Lowgrade or absent |
| Local signs | Joint swelling, effusion, limited range of motion | Tenderness over bone, possible sinus tract |
| Common sites | Hip, knee, ankle (synovial joints) | Long bones (femur, tibia), pelvis, humerus |
| Lab clues | Very high WBC, CRP, ESR; positive joint fluid culture | Elevated CRP/ESR; blood cultures less frequent |
So, how do you differentiate between septic arthritis and osteomyelitis clinically? Look for rapid swelling of a specific joint, a high fever, and an inability to move the joint without painthat screams septic arthritis. If the pain is more diffuse, creeping along the length of a bone, and the fever is modest, osteomyelitis is more likely.
Let me share a quick story. A friend of mine, Sam, went to the ER after his knee suddenly locked up with intense pain and a fever of 103F. The doctor tapped the joint, drained a cloudy fluid, and started antibiotics within hoursclassic septic arthritis. Two weeks later, my cousin Maya complained of a dull ache in her shin that lingered for months after a minor cut. Imaging showed a sequestrum, and she needed surgical debridementdefinitely osteomyelitis. Those realworld moments illustrate why the clinical picture matters.
Imaging and Radiology
When the physical exam leaves you guessing, imaging steps in as the ultimate truthtester. Xrays are often the first look, but they may only show late changes. MRI is the gold standard for both conditions, revealing bone marrow edema, joint effusion, and the subtle differences that separate a joint infection from a bone infection.
Septic arthritis on MRI usually shows a joint effusion with synovial membrane enhancement and marrow edema limited to the epiphysis (the end of the bone where the joint sits). Osteomyelitis displays a more extensive patterncortical destruction, a sequestrum (dead bone), and an involucrum (new bone forming around it). If you search for septic arthritis vs osteomyelitis radiology, youll see sidebyside pictures that make the distinction crystal clear.
According to a study in the database, MRI can pinpoint septic arthritis within the first 2448hours, whereas plain films may take weeks to reveal osteomyelitis signs. Thats why doctors often order an MRI early when the stakes are high.
Lab Tests and Microbiology
Laboratory work is the silent partner that confirms what imaging suggests. For septic arthritis, the definitive test is a joint aspirationpulling fluid from the joint and sending it to the lab. The fluid is usually cloudy, with a white cell count exceeding 50,000 cells/L, and cultures often grow Staphylococcus aureus, the most common culprit.
Osteomyelitis, by contrast, often relies on a bone biopsy, especially if blood cultures come back negative. The same bacteria dominate, but youll also see Gramnegative bacilli or, in kids, Kingella kingae. Knowing the pathogen guides the choice of antibioticsMRSAactive agents for resistant S. aureus, for instance.
Treatment Strategies Overview
Septic Arthritis Management
The first rule with septic arthritis is drain it fast. Whether its needle aspiration, arthroscopy, or an open washout, removing the infected fluid saves the joint. After drainage, highdose intravenous antibiotics begin immediatelyusually 24weeks, then a short oral course if the infection settles. Early physical therapy is crucial; gentle rangeofmotion exercises prevent stiffness and preserve function.
Osteomyelitis Management
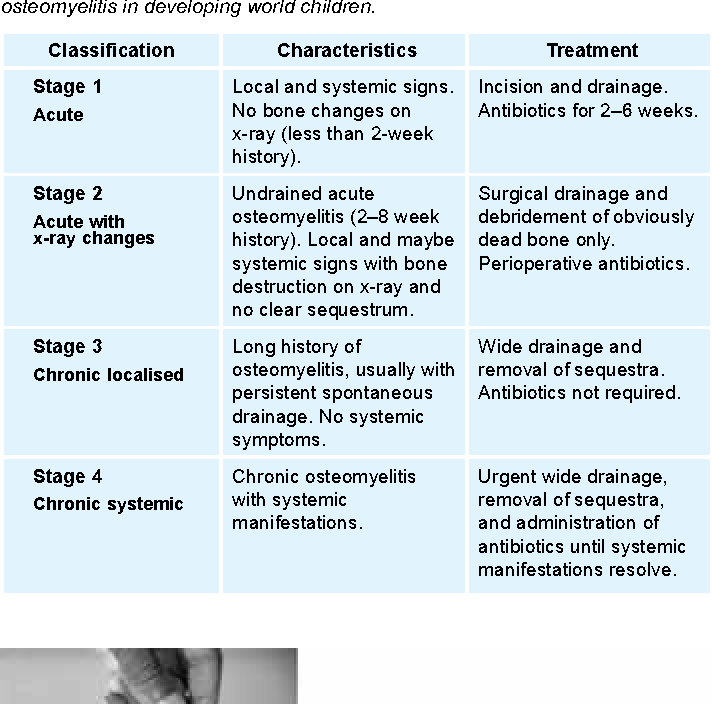
Osteomyelitis often needs a twopronged attack: surgical debridement to excise dead bone, followed by a prolonged antibiotic regimen (typically 46weeks IV). Some cases, especially earlystage pediatric infections, can resolve with antibiotics alone, but most adults require surgery to clear the infection.
Combined or Overlapping Cases
Its not uncommon for both conditions to coexistabout 1015% of patients with a joint infection also have adjacent bone involvement. In such scenarios, surgeons may perform both joint washout and bone debridement in the same operation, and cultures are taken from both sites to tailor therapy.
Treatment Algorithm
| Step | Septic Arthritis | Osteomyelitis |
|---|---|---|
| 1. Diagnose | Joint aspiration + MRI | MRI bone biopsy |
| 2. Immediate Action | Drainage (needle/arthroscopy) | Debridement if chronic |
| 3. Antibiotics | IV 24weeks oral | IV 46weeks oral |
| 4. Rehab | Early ROM, PT | Weightbearing as tolerated, PT |
| 5. Followup | CRP/ESR weekly, repeat MRI if needed | Serial CRP/ESR, repeat imaging at 68weeks |
Prognosis and FollowUp
Both infections have good outcomes when caught early, but the road to recovery differs. Septic arthritis can heal completely if the joint is drained promptly, but delayed treatment may lead to permanent cartilage loss, arthritis, or even joint fusion. Osteomyelitis, especially chronic cases, may require multiple surgeries, and in children it can affect growth plates, leading to limb length discrepancies.
Monitoring involves regular blood tests (CRP, ESR) and repeat imaging. Redflag signs that demand urgent attention include persistent fever, worsening pain despite antibiotics, or new drainage from a sinus tract. Those cues often signal a complicationlike an abscess or new infection sitethat needs surgical revision.
When to Seek Help
Never ignore a hot, swollen joint or a bone that hurts more each day. If you notice any of the following, call your doctor or head to the nearest emergency department:
- Fever above 101F with joint pain
- Rapid loss of joint movement
- Visible swelling or redness over a bone
- Recent trauma, surgery, or intravenous drug use
- Unexplained weight loss or night sweats (signs of systemic infection)
Early intervention not only speeds up recovery but also dramatically lowers the risk of severe complications. Remember, its always better to be safe and get evaluatedyour body will thank you later.
Wrapping It All Up
In a nutshell, septic arthritis strikes the joint with lightning speed and demands immediate drainage plus targeted antibiotics, while osteomyelitis creeps along the bone and often needs a blend of surgery and a longer antibiotic course. Both conditions can be dangerous, but recognizing the subtle cluesfever patterns, pain location, imaging findingshelps you and your clinician choose the right path.
If any of this resonates with something youve experienced, dont waitreach out to a healthcare professional right away. And if you have questions or stories about navigating these infections, feel free to share them in the comments. Together we can turn scary medical terms into understandable, manageable steps toward health.
For clinicians tracking infection severity and organ dysfunction in patients who progress to systemic disease, tools like the SOFA score can help guide prognosis and escalation of care.
FAQs
What are the main clinical signs that differentiate septic arthritis from osteomyelitis?
Septic arthritis usually presents with sudden, severe joint pain, high fever, swelling, and limited range of motion, whereas osteomyelitis often causes a gradual, deep bone ache, mild or no fever, and tenderness over the affected bone.
Which imaging study is considered the gold standard for both conditions?
MRI is the gold‑standard imaging modality because it can detect early joint effusion and bone marrow edema, allowing clinicians to distinguish septic arthritis from osteomyelitis within the first 24‑48 hours.
How is septic arthritis definitively diagnosed?
The definitive test is joint aspiration. The retrieved fluid is examined for a high white‑cell count (usually >50,000 cells/µL) and cultured to identify the causative organism, most commonly Staphylococcus aureus.
When is surgery required for osteomyelitis?
Surgery is generally needed for chronic osteomyelitis to remove dead bone (sequestrum) and any surrounding infected tissue. Early‑stage disease in children may sometimes be treated with antibiotics alone.
Can a patient have both septic arthritis and osteomyelitis at the same time?
Yes, about 10‑15 % of patients with a joint infection also have adjacent bone involvement. In such cases, both joint drainage and bone debridement are performed, and cultures are taken from each site to guide therapy.