Understanding Secondary Hypothyroidism
What is secondary hypothyroidism?
In plain English, secondary hypothyroidism means your thyroid gland is fine, but the pituitary gland (the master gland at the base of your brain) isnt sending the right amount of thyroidstimulating hormone (TSH) to tell the thyroid to work. Without that signal, your thyroid cant produce enough thyroid hormone, leading to the classic hypothyroid symptoms.
Common causes (secondary hypothyroidism cause)
These are the usual suspects:
- Pituitary adenomas (benign tumors)
- Surgery or radiation that affect the pituitary
- Traumatic brain injury
- Infiltrative diseases such as sarcoidosis or histiocytosis
- Sheehans syndrome (postpartum pituitary infarction)
All of these fall under the broader term pituitary hypothyroidism, which you might see used interchangeably in medical literature.
Typical symptoms (secondary hypothyroidism symptoms)
Because the thyroid hormone is low, you may notice:
- Persistent fatigue that no amount of coffee seems to fix
- Cold intoleranceeven your favorite sweater feels insufficient
- Unexplained weight gain or difficulty losing weight
- Menstrual irregularities or reduced libido
- Dry skin, hair loss, and slowed reflexes
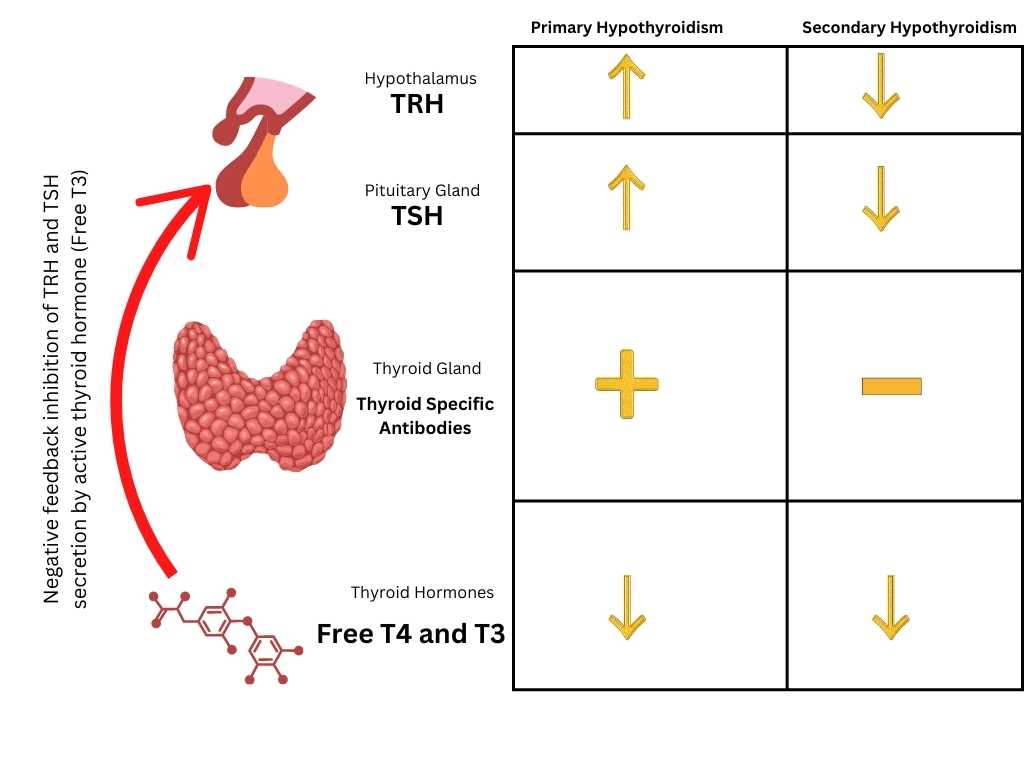
Heres a quick sidebyside look at how primary and secondary hypothyroidism differ in symptom patterns:
| Feature | Primary (thyroid problem) | Secondary (pituitary problem) |
|---|---|---|
| TSH level | High | Low or normal |
| Free T4 | Low | Low |
| Associated pituitary signs | None | Possible visual field loss, headaches, other hormone deficits |
A realworld story (experience)
Take Maya, a 42yearold graphic designer. After a transsphenoidal surgery to remove a small pituitary tumor, she started feeling offlethargic, chilly, and unusually forgetful. Her doctor ordered a thyroid panel, which showed a low free T4 with an inappropriately low TSH. The diagnosis? Secondary hypothyroidism. Mayas journey illustrates how the diagnosis often follows a bigger pituitary issue, and why paying attention to those subtle changes can be a lifesaver.
Diagnosing the Condition
Lab work what numbers matter? (secondary hypothyroidism, TSH and T4 levels)
The hallmark lab pattern is a low free T4 paired with a low or normal TSH. In primary hypothyroidism the TSH spikes, but when the pituitary is the problem, it simply cant crank up the signal.
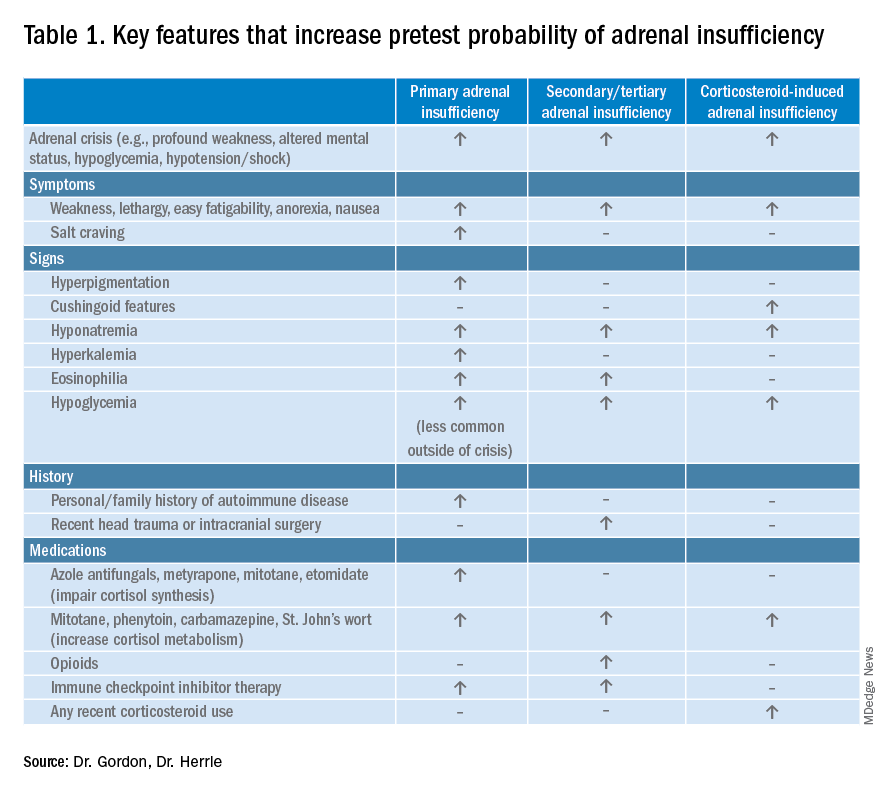
Many endocrinologists also check cortisol levels before starting thyroid hormone, because a hidden adrenal insufficiency can become dangerous once you boost metabolism. , treating both deficiencies simultaneously is crucial for safety.
Imaging & other tests
If the lab results raise suspicion, an MRI of the pituitary is the gold standard. It can reveal adenomas, postsurgical scarring, or infiltrative lesions. Occasionally, a visual field test is ordered if the tumor compresses the optic chiasm.
Sample lab report walkthrough (secondary hypothyroidism lab results)
Imagine you get a report that reads:
- TSH: 0.3IU/mL (reference 0.44.0)
- Free T4: 0.6ng/dL (reference 0.81.8)
- Morning cortisol: 7g/dL (reference 525)
The low TSH and low free T4 point straight to secondary hypothyroidism, while the borderline cortisol reminds the clinician to keep an eye on adrenal function.
Core Treatment Principles
Goal of therapy replace the missing hormone
Simply put, we aim to give your body the thyroid hormone its missing, without overloading it. Levothyroxine (synthetic T4) is the goto drug because it mimics the natural hormone the thyroid would have made.
Firstline medication (secondary hypothyroidism treatment)
Most guidelinesincluding those from the American Association of Clinical Endocrinologistsrecommend starting with a weightbased dose of about 1.51.8g per kilogram of body weight per day. That translates to roughly 100150g for an average adult.
According to a study in the , the key is the lowest effective dose to avoid overtreatment symptoms like rapid heartbeats or bone loss.
How levothyroxine works across primary, secondary & tertiary forms (pituitary hypothyroidism treatment)
Levothyroxine is absorbed mainly in the small intestine and converted to the active hormone T3 inside cells. Food, calcium supplements, and iron can hinder absorption, so its best taken on an empty stomachusually 3060 minutes before breakfast.
Dosing algorithm (stepbystep)
- Calculate starting dose: weight (kg) 1.6g = initial daily dose.
- Check labs in 68weeks: look at free T4 (primary target) and TSH (secondary check).
- Adjust dose: increase or decrease by 1225g based on lab trends and symptoms.
- Stabilize: once free T4 sits in the middle of the reference range and symptoms improve, recheck every 612months.
Balancing benefits & risks (trustworthiness)
Benefits:
- Restores energy levels and mental clarity
- Normalizes metabolism, aiding weight management
- Improves mood, menstrual regularity, and overall quality of life
Risks of overreplacement:
- Palpitations, anxiety, insomnia
- Potential bone density loss with longterm high doses
- Elevated serum TSH may mask underlying pituitary problems
Because the stakes are personal, the best approach is a shared decisionmaking conversation with your endocrinologist.
Special situations
Pregnancy
During pregnancy, the demand for thyroid hormone rises by about 30%. Many women need a 2050% dose increase, and free T4 must be monitored every 46weeks. Untreated hypothyroidism can affect fetal brain development, so close collaboration with obstetrics is essential.
Children & adolescents
Kids with secondary hypothyroidism usually require lifelong treatment, but dosing is based on weight and growth velocity. Regular pediatric endocrine followup ensures that growth milestones stay on track.
Concomitant adrenal insufficiency
If your labs show low cortisol, doctors will start glucocorticoid replacement before levothyroxine. Jumpstarting thyroid hormone without adequate cortisol can trigger an adrenal crisisa medical emergency.
Monitoring & FollowUp
Lab schedule after starting therapy
The typical timeline looks like this:
- 68weeks: First recheck of free T4 (primary target)
- 12weeks: Confirm stability; adjust dose if needed
- Every 612months: Once stable, routine labs keep you in the sweet spot
Signs that dose needs tweaking
Even with perfect labs, you might feel off. Watch for:
- Persistent fatigue or new weight gain
- Heart racing, tremors, or insomnia (possible overtreatment)
- Changes in mood or menstrual patterns
Patientdriven tools
Keeping a simple log can save trips to the doctor. Print a Medication & Lab Log template and note:
- Date of dose change
- Free T4 and TSH results
- Symptom rating (110)
- Any interfering supplements (calcium, iron)
There are also several free smartphone apps that send reminders and let you chart trends over time.
Expert Insights & Resources
For a deeper dive, consider the following trusted sources:
- UCLA Healths endocrine patient guide (excellent for dosing nuances)
- American Thyroid Association (ATA) treatment guidelinesespecially the section on secondary hypothyroidism
- Merck Manuals concise overview of pituitary hypothyroidism
When you read these resources, youll notice a consistent emphasis on individualized care, regular monitoring, and the importance of checking other pituitary hormonesexactly the balanced approach weve championed here.
Conclusion
Secondary hypothyroidism can feel like a maze, but with the right information and a collaborative doctorpatient partnership, the path becomes clear. Hormone replacementmost often levothyroxinetailored to your labs, weight, and life circumstances, is the cornerstone of treatment. By understanding the cause, recognizing the symptoms, and staying on top of followup labs, youll keep your thyroid function in the just right zone without unnecessary risk.
Remember, youre not alone on this journey. If you have questions, want to share how your treatment plan is working, or simply need a friendly ear, drop a comment below or join a support community. Your experience can help someone else navigate the same road. Heres to feeling balanced, energized, and empowered!
FAQs
What is the main difference between primary and secondary hypothyroidism?
Primary hypothyroidism is caused by a problem in the thyroid gland itself, leading to high TSH levels. Secondary hypothyroidism originates from insufficient TSH production by the pituitary, so both TSH and free T4 are low.
How is levothyroxine dosage determined for secondary hypothyroidism?
Doctors usually start with a weight‑based dose of about 1.5‑1.8 µg per kilogram per day (roughly 100‑150 µg for most adults) and then adjust every 6‑8 weeks based on free T4 levels and symptoms.
Why must cortisol levels be checked before starting thyroid hormone therapy?
Low cortisol (adrenal insufficiency) can become life‑threatening when metabolism is increased by thyroid hormone. Replacing cortisol first prevents an adrenal crisis.
Can secondary hypothyroidism treatment be adjusted during pregnancy?
Yes. Hormone needs rise about 30 % in pregnancy, so the levothyroxine dose often needs to be increased and free T4 monitored every 4‑6 weeks to protect both mother and baby.
How often should lab tests be performed after beginning treatment?
The first re‑check is typically at 6‑8 weeks to assess free T4. Subsequent labs are done at 12 weeks, then every 6‑12 months once the dose is stable.