What Are Rome Criteria
Ever wonder why some patients with chronic back pain get flagged for ankylosing spondylitis (AS) even when their Xrays look perfectly normal? Thats the magic of the Rome criteria for ankylosing spondylitis. In plain English, these criteria are a checklist of clinical clues that help doctors suspect AS when the classic sacroiliac (SI) joint images dont show the usual damage.
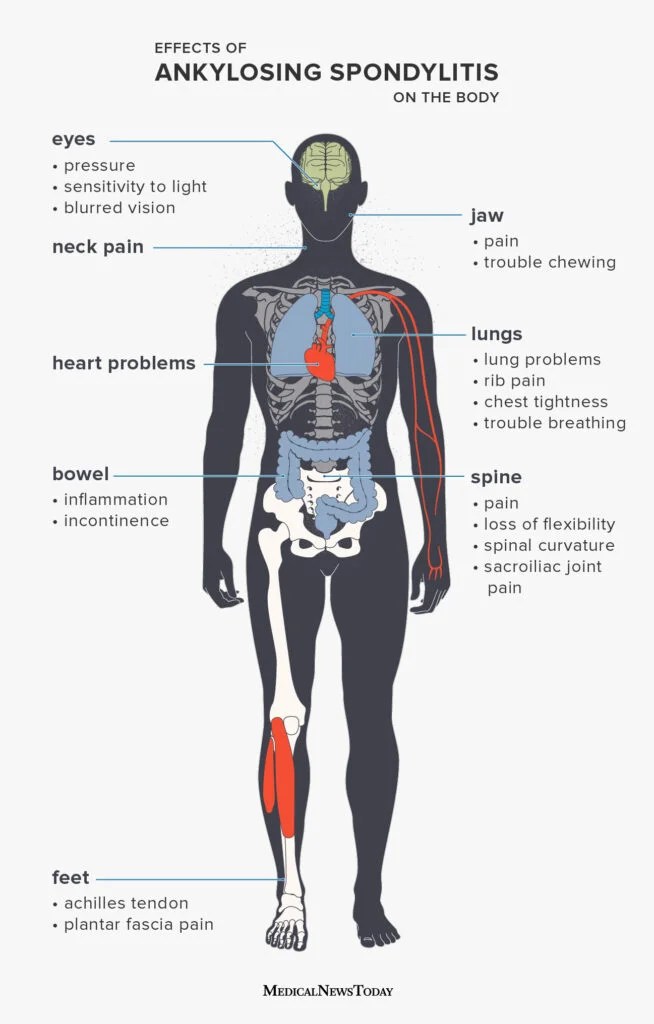
Back in 1961, a group of rheumatologists gathered in Rome and said, Lets not rely solely on Xrays; we need a way to catch early disease based on what patients actually feel. The result was a set of symptomspersistent inflammatory lowback pain, improvement with exercise, limited chest expansion, and a few extra extras like uveitis or heel painthat can point to AS even if the SI joints appear untouched.
Rome vs Other Systems
When you search for ankylosing spondylitis classification criteria, youll quickly bump into the ASAS criteria, the NewYork criteria, and the modified NewYork criteria. How do they stack up?
| Criterion | Primary Focus | Imaging Needed | Typical Sensitivity |
|---|---|---|---|
| Rome (1961) | Clinical symptoms only | None (Xray optional) | 65% |
| NewYork (1984) | Radiographic sacroiliitis + clinical | Pelvic Xray required | 73% |
| Modified NewYork (1990) | Same as NewYork, stricter cutoffs | Pelvic Xray | 78% |
| ASAS (2009) | Axial spondyloarthritis (clinical + MRI) | MRI or Xray | 85% |
Notice how the Rome criteria rely purely on what the patient tells you and what you can test in the exam room. That makes them a great firstline screen, especially in primarycare settings where MRI isnt always on tap.
Applying Rome In Practice
If youre a clinicianor just someone trying to understand what your doctor might be looking forheres a quick, stepbystep rundown of how to use the Rome criteria.
Who Should Be Screened?
Picture a 28yearold who wakes up with a stiff lower back that feels better after a morning jog but never fully eases up. If that pain has stuck around for at least three months, it ticks the first box of the Rome checklist.
Clinical Checklist
- Inflammatory lowback pain 3months (worse at night, improves with movement)
- Improvement with exercise, not rest
- Limited lumbar flexion (forward bend)
- Limited chest expansion (<2.5cm reduction)
- Peripheral arthritis (especially in hips or knees)
- Enthesitis (heel pain at the Achilles insertion)
- Acute anterior uveitis episodes
Scoring The Checklist
While the original Rome paper didnt assign points, many clinics now give one point per feature and consider a score of4or more Romepositive. This simple math helps keep the assessment objective.
RealWorld Example
John, a 32yearold graphic designer, visited his primarycare doctor after six months of persistent morning stiffness. His Xray came back normal, but the exam revealed limited chest expansion and heel tenderness. He scored five points on the Rome checklist, prompting a referral for an MRI. The MRI later showed early sacroiliitis, confirming AS.
Benefits and Risks
Like any medical tool, the Rome criteria have bright sides and shadows. Lets weigh them together.
Benefits
- Early detection: Spotting AS before Xray changes appear can fasttrack treatment and potentially slow disease progression.
- Costeffective: No need for expensive imaging right away.
- Accessible: Any clinician can apply the checklist during a routine exam.
Risks & Limitations
One major drawback is sensitivity. A study in Arthritis & Rheumatology found that about onethird of early AS patients are missed if we rely solely on the Rome criteria. In other words, normallooking Xrays and a borderline clinical picture can still mask disease.
Theres also a risk of overreliance: if a doctor says Your Xray is fine, youre okay, without considering the Rome checklist, a patient could wait months for the right referral. Thats why most experts suggest using Rome as a gateway, then confirming with the newer ASAS criteria or MRI when uncertainty persists.
Imaging Insights Today
When the Rome criteria raise suspicion, the next logical step is imagingusually an MRI of the sacroiliac joints. Why? Because MRI can spot inflammation and bonemarrow edema long before a plain Xray shows erosion.
What Normal SI Joints Look Like
In the modified NewYork system, sacroiliitis is graded from 0 (normal) to 4 (complete ankylosis). A normal reading means the radiologist sees no visible erosions, sclerosis, or joint space narrowing. Thats exactly the scenario where the Rome criteria shine: they catch patients who feel the disease even though their Xray score is 0.
When To Order MRI
- Persistent inflammatory back pain >6months
- Elevated inflammatory markers (CRP or ESR)
- Family history of spondyloarthritis
- Positive Rome criteria score (4)
In practice, an MRI report might read, Bonemarrow edema in bilateral sacroiliac joints compatible with active sacroiliitis, confirming the clinicians suspicion. If the goal is to assess treatment response and sustained improvement, many clinicians will then evaluate for ankylosing spondylitis remission using formal remission criteria alongside imaging.
Trusted Sources & Reading
To feel confident about what youre reading, it helps to know where the information comes from. Here are a few goto references that many rheumatologists rely on:
These sources not only provide evidencebased data but also showcase why the Rome criteria still matter in todays diagnostic landscape.
Conclusion
So, whats the bottom line? The Rome criteria for ankylosing spondylitis are a handy, lowcost, and surprisingly effective way to spot early disease when imaging looks clean. Their strength lies in focusing on what the patient actually feelsthose stubborn morning stiffnesses, the relief that comes with a jog, and the subtle loss of chest expansion.
But remember, theyre not a silver bullet. Pairing the Rome checklist with modern tools like MRI and the ASAS criteria gives you the best shot at catching AS early, starting treatment sooner, and hopefully keeping the disease from stealing your flexibility.
Got a story about how a simple clinical clue led to a diagnosis? Or maybe youre curious whether you should ask your doctor about the Rome criteria? Drop a comment, share your experience, or simply ask a questionlets keep the conversation going. After all, knowledge shared is pain eased.
FAQs
What are the Rome criteria for ankylosing spondylitis?
They are a set of clinical signs—such as inflammatory low‑back pain, improvement with exercise, limited chest expansion, and extra‑articular features—that help identify early ankylosing spondylitis without relying on X‑ray changes.
How do the Rome criteria differ from the New York or ASAS criteria?
The Rome criteria use only clinical findings, while the New York and modified New York criteria require radiographic sacroiliitis, and the ASAS criteria add MRI findings to the clinical picture.
When should a clinician apply the Rome checklist?
Screen any adult under 45 with chronic inflammatory low‑back pain lasting ≥ 3 months, especially when X‑rays are normal but symptoms suggest spondyloarthritis.
What is the recommended next step if a patient scores positively on the Rome criteria?
A positive score (usually ≥ 4 points) should prompt referral for MRI of the sacroiliac joints and further rheumatology evaluation to confirm or rule out ankylosing spondylitis.
Can the Rome criteria miss early ankylosing spondylitis cases?
Yes. Sensitivity is about 65 %, so some early cases may be missed; therefore, clinicians often combine Rome with newer imaging‑based criteria for higher diagnostic accuracy.