FAQs
What are the most common risk factors for preterm labour according to RCOG?
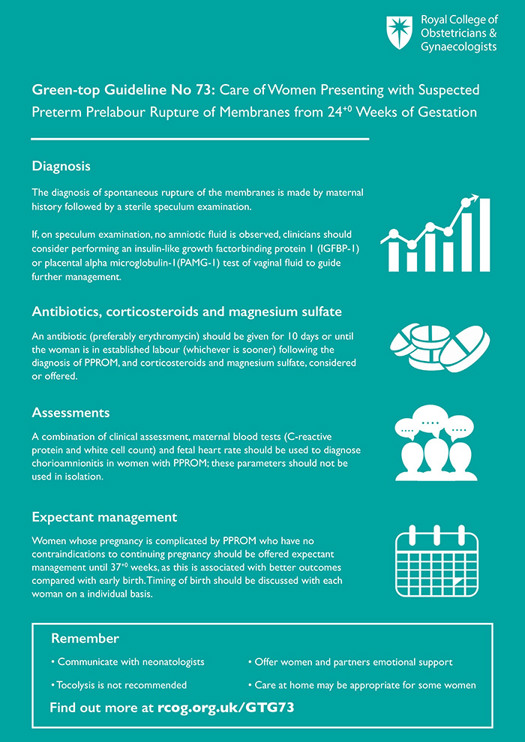
RCOG highlights several key predictors: previous pre‑term birth, short cervical length (<25 mm) early in pregnancy, chronic hypertension or pre‑eclampsia, multiple gestation, uterine anomalies, smoking, alcohol use, and certain infections.
How does a short cervical length increase the chance of preterm labour?
A short cervix indicates that the structural support of the uterus is reduced, allowing the cervix to efface and dilate earlier under the weight of the pregnancy. Each millimetre below the 25 mm threshold raises the risk of uterine contractions and early delivery by about 5‑10 %.
Can progesterone therapy prevent preterm labour, and who should use it?
Yes. Daily vaginal progesterone (200 mg) from 16 weeks to 36 weeks significantly cuts the risk of early delivery—especially for women with a short cervix or a history of pre‑term birth. It is recommended by RCOG and NICE as a first‑line prophylactic treatment.
When should I ask my doctor for a cervical‑length scan?
Schedule a trans‑vaginal cervical‑length scan at 12‑14 weeks if you have any of the following: previous pre‑term birth, chronic hypertension, uterine structural anomalies, prior cervical surgery (e.g., conisation), or a family history of early labour.
What should I do if I experience early signs of labour before 37 weeks?
Contact your maternity team immediately. Follow the RCOG protocol: they may give corticosteroids for fetal lung maturity, start tocolytic medication (often nifedipine) to delay labour for 48‑72 hours, and arrange transfer to a tertiary centre if needed.