Rett syndrome is caused by a mutation in the MECP2 gene on the X chromosome. In other words, the chromosome number that matters here is the X chromosome the same one that determines gender in humans.
Knowing this matters because it explains why girls are affected far more often than boys, guides genetic testing, and helps families understand inheritance patterns, prognosis, and the care options that are available.
Quick Genetics Snapshot
What is the MECP2 gene?
The MECP2 gene lives on a specific region of the X chromosome called Xq28. Think of it as a tiny instruction manual that tells cells how to read other genes correctly. When this manual is damaged, the whole library of genetic information can get a little chaotic, leading to the neurological challenges we see in Rett syndrome.
What does chromosome number actually mean?
Humans have 23 pairs of chromosomes 22 pairs that look the same in both sexes (autosomes) and one pair that decides sex: X and Y. When we talk about the rett syndrome chromosome number, we're simply zeroing in on the X chromosome that carries the MECP2 mutation.
How many chromosomes are involved in Rett?
Only the X chromosome carries the pathogenic variant. No other chromosome number plays a direct role in causing the disorder, although other genetic factors can sometimes influence severity.
Key Point
All credible sources confirm that Rett syndrome is an X-linked condition. For families seeking treatment navigation or support programs related to therapies, there are assistance resources available for specific therapies like Exondys 51 assistance that can help with cost and access for eligible patients: Exondys 51 assistance.
Inheritance and Risk
Is Rett syndrome dominant or recessive?
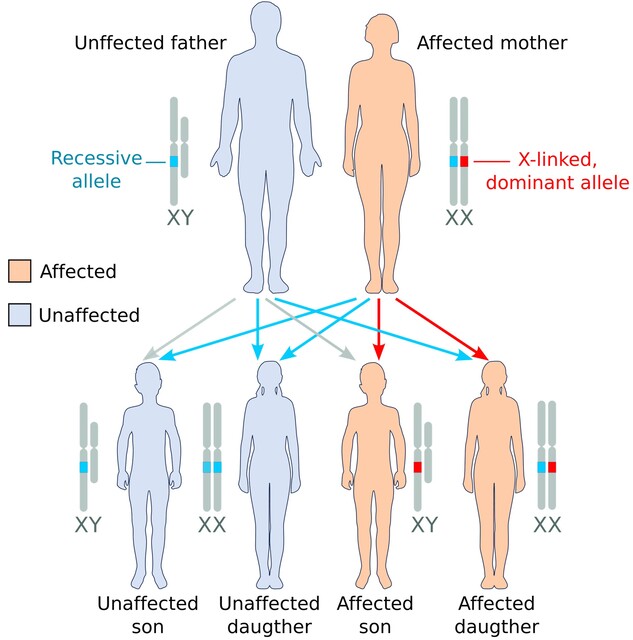
Even though it's X-linked, the mutation acts dominantly on the X chromosome. That means a single altered copy of MECP2 in a girl is enough to cause the syndrome, because she has two X chromosomes and one faulty copy will dominate the normal copy.
Why are females affected more than males?
Girls have two X chromosomes, so even if one carries the mutation, the other can partially compensate. Boys, on the other hand, have only one X; a mutation there often leads to more severe outcomes, sometimes even fetal loss. This is why you'll see the phrase Rett syndrome X-linked pop up in most articles.
What is a de novo mutation?
More than 95% of Rett cases arise from a brand-new (de novo) change in the MECP2 gene meaning the parents' DNA looks perfectly normal. Researchers have traced many of these fresh mutations back to a single cell error during early embryonic development.
Real-World Example
Sarah, a mother of two, thought her youngest daughter's developmental pause was just a phase. After a pediatrician noticed hand-wringing and recommended genetic testing, the MECP2 mutation was confirmed. Sarah's story echoes countless families who discover a de novo mutation after months of uncertainty.
Clinical Picture Overview
Core Rett symptoms
Typical signs begin after a period of apparently normal development (618 months). Expect to see:
- Loss of purposeful hand use
- Repetitive hand-wringing or clapping
- Speech regression (often to a few words)
- Gait abnormalities a shuffling walk or toe-walking
- Seizures in up to 80% of cases
Facial features and other clues
While no single facial trait is diagnostic, many children display a small head (microcephaly), a flattened midface, or a high-arched palate. These cues can help clinicians suspect Rett early on.
Life expectancy and long-term outlook
Thanks to better nutrition, seizure management, and supportive therapies, many individuals now live well into their 40s or 50s. A recent cohort study reported a median life expectancy of around 58 years, a marked improvement from earlier decades.
Table: Typical Symptom Timeline
| Age Range | Typical Signs |
|---|---|
| 06 months | Normal growth, early motor milestones |
| 618 months | Onset of regression: loss of hand skills, speech slowdown |
| 14 years | Hand-wringing, gait abnormalities, emergence of seizures |
| 5 years+ | Stabilization of motor abilities, increased need for communication supports |
Diagnosis and Testing
Genetic testing options
The gold standard is targeted sequencing of the MECP2 gene. Many labs now offer a Rett-specific panel that also checks for CDKL5 and FOXG1, genes linked to Rett-like presentations.
Does a standard karyotype help?
A classic chromosome karyotype looks at the whole set of chromosomes but won't spot the tiny point mutation in MECP2. It can, however, rule out larger chromosomal rearrangements that might mimic Rett symptoms.
When should you suspect Rett and get tested?
If you notice a toddler who suddenly stops using words, starts repetitive hand movements, or shows a regression after an initial burst of development, it's time to talk to a pediatric neurologist about genetic testing. Early diagnosis opens doors to early intervention, speech therapy, and seizure management.
Pro Tip
Keep a simple symptom checklist at home it's easier to discuss concrete observations with your doctor than vague concerns.
Rett Prevalence Stats
How common is Rett syndrome?
Worldwide, Rett syndrome occurs in approximately 1 in 10,000 to 15,000 live female births. The numbers are fairly consistent across populations, though some registries hint at slight regional variations.
Geographic or ethnic differences?
Current research indicates there isn't a strong ethnic bias. Most large-scale studies show a similar prevalence in North America, Europe, and Asia.
Impact on family planning
Because most cases are de novo, the recurrence risk for future children is low (about 1%). However, families with an identified carrier (a parent with a mild MECP2 variant) should consider genetic counseling before expanding their family.
Quick Reference Table
| Metric | Estimate |
|---|---|
| Birth prevalence (girls) | 1 in 10,00015,000 |
| Male prevalence | Rare (often more severe) |
| De novo mutation rate | 95% |
| Average life expectancy | 58 years (modern data) |
Practical Takeaway Guide
Checklist for parents and caregivers
- Monitor developmental milestones closely note any regression.
- Ask your pediatrician about MECP2 genetic testing if red flags appear.
- Engage with early-intervention services: speech, occupational, and physical therapy.
- Stay on top of seizure control half of children need medication.
- Connect with support groups; shared experiences can be a lifeline.
Trusted resources you can rely on
When you need reliable, up-to-date information, turn to organizations that are actively funded and research-driven. For questions about insurance coverage for treatments and therapies related to rare neurological conditions, resources that explain Exondys 51 insurance options may be helpful for families navigating payer policies: Exondys 51 insurance.
Emerging research you might hear about
Scientists are exploring gene-therapy approaches that aim to replace the faulty MECP2 protein. Early-phase trials have shown promise in mouse models, and human studies are on the horizon. While it's still experimental, the optimism in the research community is palpable.
Remember
Understanding that Rett syndrome hinges on a single chromosome the X gives you a clear lens through which to view genetics, inheritance, and care strategies. It doesn't solve every challenge, but it empowers you with knowledge and direction.
Conclusion
In a nutshell, Rett syndrome is an X-linked neurodevelopmental disorder caused by a mutation in the MECP2 gene on the X chromosome. This single chromosome number shapes how the disease shows up, why girls are primarily affected, and how families can navigate diagnosis, treatment, and long-term planning. Armed with accurate genetics, realistic expectations about life expectancy, and a toolbox of supportive resources, you can advocate more confidently for yourself or a loved one. If you have questions, reach out to a genetic counselor, join a community forum, or simply share your story in the comments below. Together, we turn knowledge into hope.