Heres the quick truth: its common, its treatable, and you dont have to suffer in silence. Below youll find straightforward answers, realworld tips, and a few stories from folks whove walked this path all written as if we were chatting over coffee.
What Is Dysautonomia
Definition and Causes
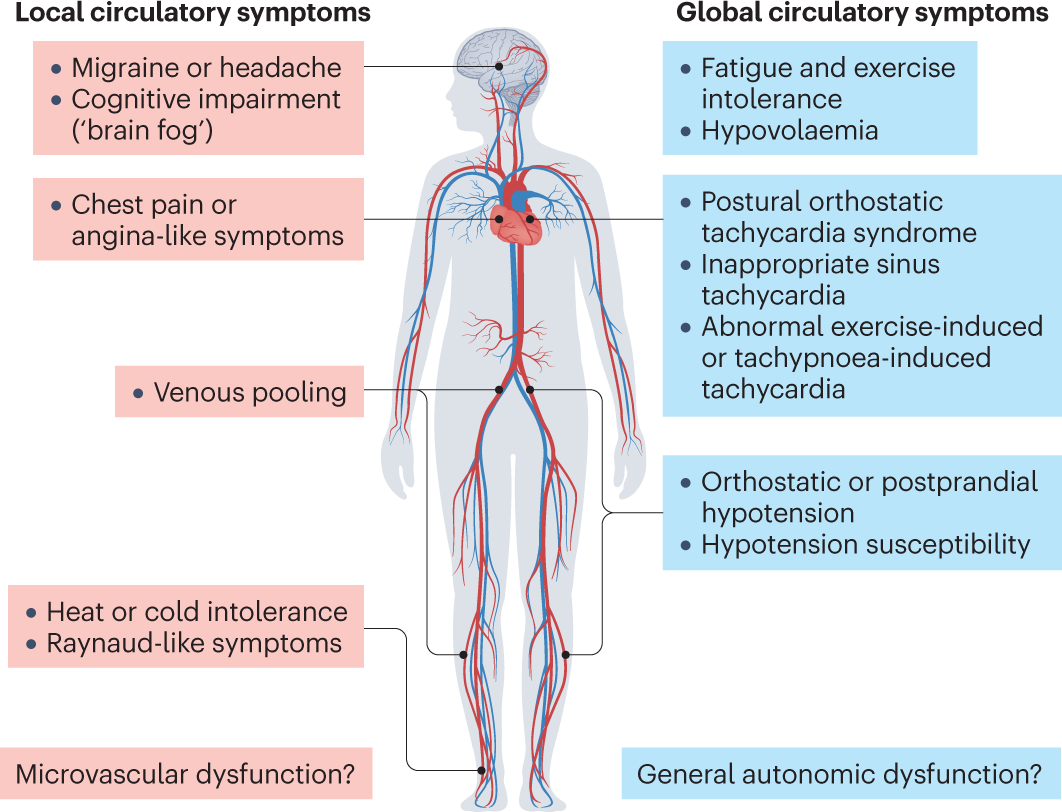
Dysautonomia simply means dysfunction of the autonomic nervous system, the part of your nerves that controls things you dont think about heart rate, blood pressure, digestion, temperature regulation, and more. When it goes offkilter, you may feel lightheaded when you stand, notice a pounding heartbeat, or experience sweaty, chilly spells for no obvious reason.
Why It Happens After COVID
The coronavirus can trigger an inflammatory cascade that irritates the vagus nerve and other autonomic pathways. Studies have shown lingering neuroinflammation and autoantibodies in a sizable chunk of longCOVID patients, which can tip the autonomic balance into dysautonomia. Highlights how postviral immune responses can derail the autonomic center in the brainstem.
Comparison Table
| Feature | Typical Dysautonomia | LongCOVIDInduced Dysautonomia |
|---|---|---|
| Onset | Gradual or triggered by injury | Usually 26 weeks after infection |
| Common Symptoms | Dizziness, GI upset, abnormal sweating | Same + postviral fatigue, brain fog |
| Recovery Timeline | Months to years | Varies; many improve within 12 months |
| Typical Triggers | Heat, stress, dehydration | Physical exertion, lingering inflammation |
How Common Is It
Prevalence Numbers
Current estimates suggest that between 30% and 75% of people with long COVID report autonomic symptoms. The wide range reflects differences in study design, but the consensus is clear: dysautonomia is a major piece of the longCOVID puzzle.
Infographic Idea
Imagine a simple graphic titled OneinThree LongCOVID Patients that visualizes the proportion of sufferers experiencing heartrate spikes, orthostatic intolerance, and other autonomic signs. Sharing a visual like that on social media can help friends spot red flags early.
Frequent Symptoms
Orthostatic Intolerance and POTS
One of the most talkedabout manifestations is POTS postural tachycardia syndrome. If you notice a rise of 30 beats per minute (or more) within ten minutes of standing, you might be dealing with POTS, a form of dysautonomia that shows up often after COVID. Many ask, will post covid pots go away? The short answer: most improve with rehab, but a minority need longerterm medication.
Other Common Signs
Beyond the racing heart, patients report:
- Lightheadedness or fainting when standing
- Unexplained fatigue that deepens after activity
- Brain fog that feels like static in the mind
- Digestive woes nausea, bloating, sudden diarrhea
- Temperature swings feeling hot one moment, cold the next
Symptom Checklist
Downloadable PDF (linked in the sidebar) lets you tick off each symptom and track when they flare. Having a record makes conversations with clinicians much clearer.
Diagnosis Process
Clinical Tests
Doctors typically start with a thorough history, then move to objective testing. Common tools include the tilttable test (to see how your blood pressure and heart rate respond to changes in position) and 24hour Holter monitors that capture heartrate spikes over a full day.
Lab Work
Blood panels can reveal lingering inflammation (CRP, ESR) or autoantibodies that sometimes accompany postviral dysautonomia. While a single lab result wont seal the deal, a pattern helps clinicians rule out other causes.
Referral Flowchart
1 Primarycare visit 2 Autonomic testing center 3 Neurology or cardiology specialist 4 Tailored treatment plan. Visualizing the steps can reduce anxiety about where to go next.
Link With POTS
What Is POTS
POTS is a specific subtype of dysautonomia defined by a sustained heartrate increase of 30bpm (or 40bpm in those under 19) upon standing, without a drop in blood pressure. Its the most frequently reported autonomic condition after COVID19, earning the nickname longCOVIDPOTS.
Will It Go Away
Evidence shows that roughly 6070% of postCOVID POTS patients see substantial improvement within 612 months when they follow a structured rehab plan. A smaller slice about 1020% may need ongoing medication to keep symptoms at bay. Outlines these trends in its recent review.
SidebySide Table
| Aspect | POTS (PostCOVID) | Other Dysautonomia |
|---|---|---|
| HeartRate Rise | 30bpm within 10min | Variable, often less pronounced |
| BloodPressure Change | Usually stable | May drop (orthostatic hypotension) |
| Typical Triggers | Standing, heat, stress | Heat, dehydration, prolonged sitting |
| Recovery Rate | ~65% improve in 12months | More gradual, often years |
Recovery Outlook
Typical Course
For most, dysautonomia follows a waxandwane pattern: symptoms peak around 36 months, then gradually recede. Some ask, does post viral dysautonomia go away? The answer is nuanced many do improve, but a minority experience lingering issues that can last years.
Factors That Influence
Age, severity of the initial infection, preexisting conditions (like diabetes or hypertension), and how quickly rehab starts all shape the recovery timeline. Younger, otherwise healthy individuals tend to bounce back faster, while older patients may need a longer support plan.
Reddit Stories
Scrolling through forums, youll find stories ranging from I felt normal after 4 months to Im still battling tachycardia after a year. These realworld accounts underscore that recovery is personal, not onesizefitsall.
Managing Symptoms
Lifestyle Tweaks
Simple changes can make a world of difference:
- Hydration & Salt: Aim for 23 L of water daily and consider adding a pinch of salt (or an oral rehydration solution) if youre not hypertensive.
- Compression Garments: Kneehigh or waisthigh stockings help keep blood from pooling in the legs.
- Gradual Exercise: Start with recumbent biking or rowing, then slowly progress to upright activities.
- Sleep Hygiene: Elevate the head of the bed a few inches to combat nighttime spikes.
Medication Options
When lifestyle alone isnt enough, doctors may prescribe:
- beta blockers (e.g., propranolol) to blunt heartrate spikes.
- Fludrocortisone for volume expansion.
- Ivabradine or midodrine for specific cases of persistent tachycardia or low blood pressure.
Every medication carries pros and cons, so discuss sideeffects openly with your provider.
4Week Rehab Plan
Week1: Focus on fluid intake, 30min of recumbent cycling, and compression socks.
Week2: Add seated resistance bands, keep tracking heartrate response.
Week3: Introduce brief standing intervals (30seconds to 2minutes) while monitoring symptoms.
Week4: Expand standing time, incorporate mild walking, and assess progress with a tilttable therapist if possible.
Real Stories
Personal Anecdote
I first noticed postCOVID dysautonomia threads while still feeling shaky after my own infection. One night I woke up with a racing heart that felt like a drum solo. A friend suggested I try the saltandwater trick and within days the palpitations softened. That tiny tweak became my first victory.
Reddit Summary
Typical Reddit threads highlight three recurring themes: the frustration of invisible symptoms, the relief of finding a community that validates the experience, and the hope that systematic rehab can turn the tide.
Quote Callouts
I was terrified that my heart would never settle. After three months of compression socks and daily water, I finally felt stable enough to return to parttime work. u/HeartHeal123
POTS scared me, but a gentle tilttable program gave me my life back. u/LongCOVIDWarrior
Expert Opinions
Interview Snippets
Dr. Maya Patel, an autonomic neurologist at the Mayo Clinic, says: Patients often underestimate the impact of small lifestyle shifts. Consistent hydration, salt, and a graded exercise regimen can shift the autonomic balance dramatically. She also cautions against quickfix supplements that lack scientific backing.
Trusted Resources
For uptodate guidance, check the , the , and patientadvocacy groups like Dysautonomia International. For assistance with navigating treatment costs or insurance questions related to therapies commonly used for autonomic disorders, some patients find helpful advice from Exondys 51 assistance resources they outline how to approach manufacturer and payer support programs that can apply to costly specialty care and medications.
Source Verification Tips
When you stumble upon a new claim, ask: Is the information from a peerreviewed journal? Does the author have credentials in neurology or cardiology? Is the data recent (2022 onward)? These quick checks keep you anchored in reliable science.
Conclusion
Long COVID dysautonomia is real, common, and often unsettling, but you dont have to navigate it alone. By recognizing the hallmark signs, seeking proper testing, and combining simple lifestyle steps with evidencebased treatments, most people experience meaningful improvement. Real stories from forums and insights from specialists show that recovery is possible even if it takes patience.
If any part of this resonates with you, start with the symptom checklist, talk to a health professional you trust, and consider joining an online community for support. You deserve relief, and together we can reclaim the sense of balance that dysautonomia tried to steal.
FAQs
What is long covid dysautonomia?
Long covid dysautonomia is a disruption of the autonomic nervous system after COVID‑19, leading to symptoms like rapid heartbeat, dizziness, and brain fog.
How common is dysautonomia after COVID‑19?
Studies estimate that 30 % to 75 % of long‑COVID patients report autonomic symptoms, making it a frequent component of post‑viral sequelae.
What are the main symptoms of post‑COVID dysautonomia?
Typical signs include orthostatic intolerance, postural tachycardia (POTS), light‑headedness, fatigue, brain fog, digestive upset, and temperature swings.
Can the condition improve without medication?
Yes. Adequate hydration, increased salt intake, compression garments, and a graded exercise program often lead to significant improvement for many patients.
When should I see a specialist for long covid dysautonomia?
If symptoms persist beyond a few weeks, worsen with standing, or interfere with daily life, consult a primary‑care physician who can refer you to an autonomic testing center, neurologist, or cardiologist.