Hey there, friend. If youve landed on this page, youre probably wondering how renal tubular acidosis (RTA) will shape your health story. The short answer? It really depends on the type of RTA you have, whats causing it, and how quickly you start the right treatment. Most folks who get diagnosed early and stick to their treatment plan end up living normal, active lives. On the other hand, untreated or hardtomanage cases can lead to kidney trouble or bone issues down the road.
Quick Answer
Renal tubular acidosis prognosis varies by type and cause, but early detection and consistent usually mean a good quality of life. Think of it like fixing a leaky faucet: the sooner you spot the drip and replace the washer, the less water youll waste.
Common Myths
Myth #1: All RTA Types Have the Same Outcome
Its easy to lump everything together because the name sounds uniform, but the reality is far messier. Distal RTA (type1) often responds well to alkali therapy, while hyporeninemic RTA (type4) can sneak in a slow march toward chronic kidney disease if the underlying diabetes or medication issue isnt addressed.
Myth #2: Feeling Fine Means the Disease Isnt Progressing
Many people feel fine for months, even years, while silent damage accumulates in the kidneys or bones. A painless process, but one that can show up later as kidney stones, bone pain, or fatigue.
| Myth | Reality (Evidence) |
|---|---|
| Same outcome for all types | Type1 usually maintains kidney function with alkali, while type4 may advance to CKD if left untreated (Cleveland Clinic, 2024). |
| No future risk if asymptomatic | Even mild proximal RTA can cause bone loss and growth delay in children (StatPearls, 2023). |
RTA Types Overview
What Are the Main Types?
There are four classic categories:
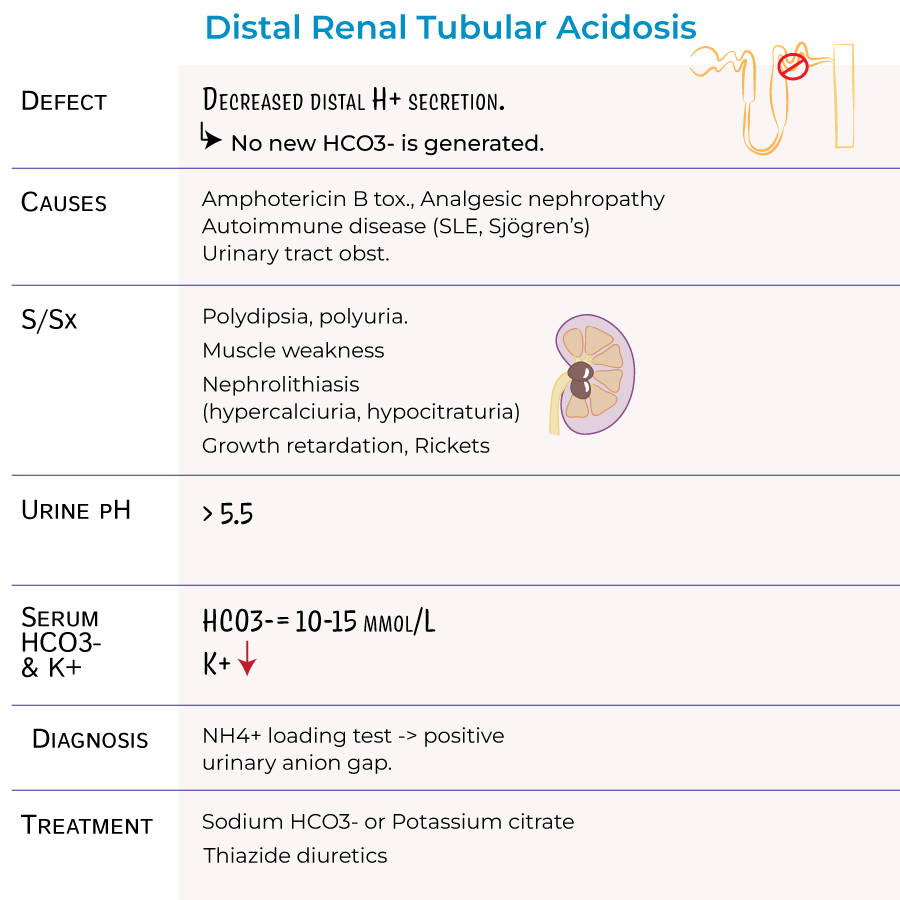
- Renal tubular acidosis type1 (Distal) the kidneys cant excrete acid properly.
- Renal tubular acidosis type2 (Proximal) the tubules cant reabsorb bicarbonate efficiently.
- Renal tubular acidosis type3 (Mixed) a rare blend of distal and proximal defects.
- Renal tubular acidosis type4 (Hyporeninemic) often tied to low aldosterone, high potassium, and diabetes.
Comparison at a Glance
| Type | Primary Cause | Lab Pattern | Key Symptoms |
|---|---|---|---|
| Type1 Distal | Genetic or autoimmune | High urine pH, low serum HCO | Kidney stones, growth failure |
| Type2 Proximal | Fanconitype tubular defect | Low serum HCO, normal urine pH early | Bone pain, glucosuria |
| Type3 Mixed | Rare inherited mutation | Features of 1+2 | Severe metabolic acidosis |
| Type4 Hyporeninemic | Diabetes, ACEI meds | Hyperkalemia, low aldosterone | Fatigue, hypertension |
Understanding which bucket you fall into is the first step toward an accurate and a realistic outlook.
Root Causes
What Triggers RTA?
Think of RTA as a traffic jam in your kidneys. The jam can be caused by:
- Autoimmune diseases (like Sjgrens)
- Medications such as ifosfamide, certain diuretics, or ACE inhibitors
- Genetic mutations that affect transporter proteins
- Chronic conditions like diabetes that impair aldosterone production
Diagnosis Criteria
A proper diagnosis follows a stepbystep flowchart:
- Blood test: Look for low serum bicarbonate (<22mmol/L) and, depending on type, altered potassium levels.
- Urine analysis: Check urine pH ( >5.5 suggests distal RTA) and the presence of glucose or amino acids (hinting at proximal dysfunction).
- Imaging: Ultrasound or CT to spot kidney stones or nephrocalcinosis.
- Genetic testing: Reserved for earlyonset or familial cases.
All these pieces together meet the renal tubular acidosis diagnosis criteria set by major nephrology guidelines.
Treatment Options
Core Therapies Tailored to Type
Each RTA type has a goto therapy, but the overarching principle is to replace the missing base and fix the underlying trigger.
- Alkali replacement Sodium bicarbonate (NaHCO) or potassium bicarbonate (KHCO) for types1 and2.
- Potassiumsparing agents Fludrocortisone or thiazide diuretics for type4.
- Addressing the cause Stopping offending drugs, treating autoimmune disease, or managing diabetes carefully.
Medication Quick Reference
| Drug | Typical Dose | Monitoring | Sideeffects |
|---|---|---|---|
| NaHCO | 0.52g three times daily | Serum bicarbonate, blood pressure | Metabolic alkalosis, volume overload |
| KHCO | 0.51g three times daily | Potassium, ECG | Hyperkalemia |
| Fludrocortisone (type4) | 0.050.2mg daily | Aldosterone, sodium | Edema, hypertension |
To keep the info solid, weve referenced the guidelines and a recent on RTA management.
Prognosis Overview
What Does the Research Say?
Lets break it down by type, because the prognosis story is different for each.
- Type1 (Distal) With steady alkali therapy, more than 95% of patients maintain normal kidney function for at least five years. The main longterm risk is kidney stones or nephrocalcinosis if urine pH stays high.
- Type2 (Proximal) If the cause is reversible (e.g., a medication), prognosis is excellent; otherwise, theres a 2030% chance of progressing to chronic kidney disease (CKD) over a decade.
- Type3 (Mixed) Because its rare, the data are scattered, but outcomes follow whichever component (distal or proximal) is most severe.
- Type4 (Hyporeninemic) Survival mirrors the underlying disease, especially diabetes. Good control of blood sugar and potassium can push fiveyear kidney survival up to 80%.
Prognosis Snapshot
| Type | 5yr Survival | 10yr Survival | Typical Complications |
|---|---|---|---|
| 1 (Distal) | >95% (treated) | >90% (treated) | Kidney stones, bone disease |
| 2 (Proximal) | 8090% (reversible) | 7080% (reversible) | Osteomalacia, growth delay |
| 3 (Mixed) | Variable | Variable | Severe metabolic acidosis |
| 4 (Hyporeninemic) | 7085% (depends on diabetes control) | 6075% (depends on diabetes control) | CKD progression, hyperkalemia |
Bottom line: early, consistent renal tubular acidosis treatment is the gamechanger that flips many of those percentages in your favor.
Prognosis Factors
What Can Shift the Outlook?
Even within the same type, several personal factors nudge the prognosis one way or another:
- Age at diagnosis Kids caught early often avoid bone complications; adults diagnosed later may already have subtle kidney damage.
- Adherence to therapy Skipping alkali doses is like letting the faucet drip; the damage adds up.
- Comorbidities Diabetes, hypertension, or chronic medication use can accelerate CKD.
- Genetics Certain mutations respond better to bicarbonate, others less so.
RealWorld Example
Emma, a 12yearold, was diagnosed with distal RTA at 6months after repeated ear infections and growth lag. Her parents started sodium bicarbonate immediately, and today she runs track, has no kidney stones, and her growth chart is back on track. Contrast that with Mark, 45, who ignored mild fatigue for years; his type4 RTA, coupled with uncontrolled diabetes, led to stage3 CKD. Both stories illustrate how timing and commitment shape the prognosis.
Helpful Resources
Downloadable Guide
Weve compiled a friendly PDF titled Living Well with RTA. It covers daily tips, medication schedules, and a symptomtracker you can print. Grab it and keep it on your fridge a visual reminder can be a lifesaver.
Trusted External Links
These sites are packed with uptodate research, patient stories, and tools that can help you navigate the journey.
Conclusion
So, whats the final takeaway? The prognosis for renal tubular acidosis isnt a onesizefitsall verdict. It hinges on the type, the root cause, andmost importantlyhow fast you and your medical team jump into action. When you catch RTA early, stick to your alkali regimen, and manage any companion conditions, youre looking at a bright, active future. If youre living with RTA, consider downloading our free PDF, share this article with anyone you think might need it, andmost cruciallychat with a kidney specialist to tailor a plan that works for you.
Wed love to hear your story. Whats been your biggest challenge with RTA? Drop a comment, ask a question, or simply let us know how youre doing. Remember, youre not alone on this road, and together we can turn a tricky diagnosis into a manageable, hopeful chapter.