Most people think Parkinsons disease only messes with movement, but the bladder can get caught in the crossfire, too. Urinary retentionwhen the bladder cant empty fullycan be a quiet, frustrating sideeffect that many overlook.
In the next few minutes well unpack why this happens, how you can spot it early, and which proven strategies (medical, lifestyle, and even simple tricks) can keep your bathroom trips under control. Think of this as a friendly chat over coffee, not a textbook lecture.
Understanding Urinary Retention
What is urinary retention?
Urinary retention is the inability to completely empty the bladder. Doctors measure it by the postvoid residual (PVR) volumeif more than 100mL of urine stays behind after you pee, that counts as retention.
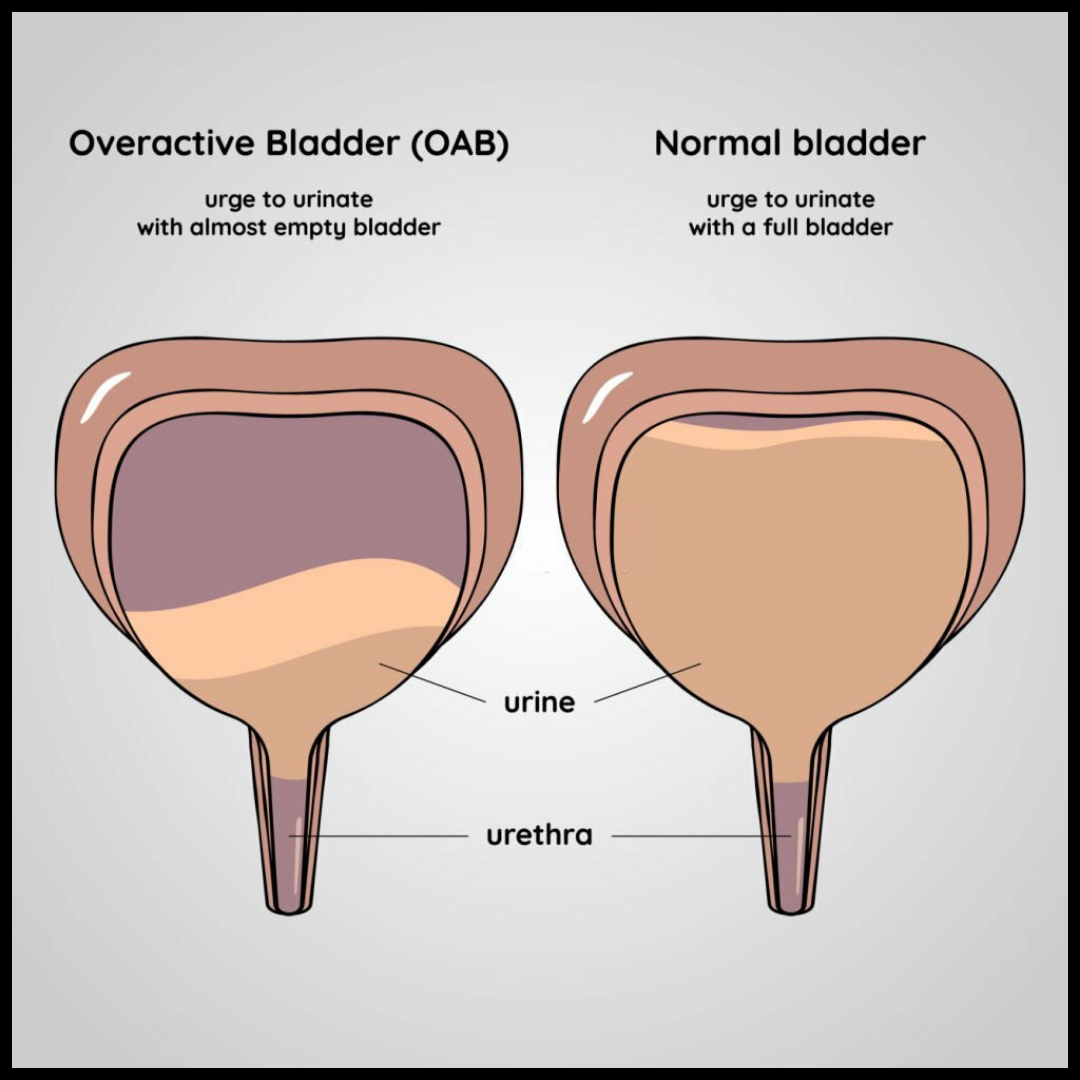
How is it different from frequent urination?
| Feature | Urinary Retention | Frequent Urination (Nocturia) | Incontinence |
|---|---|---|---|
| Core issue | Incomplete emptying | Too many trips | Leakage |
| PVR | >100mL | Normal | Normal |
| Typical cause | Neurogenic bladder | Overactive bladder, excess fluid | Weak sphincter |
How common is it?
Research shows that 3040% of people with Parkinsons report some form of bladder dysfunction. A 2022 metaanalysis found that 19% of patients under 65 and 37% over 65 experience retention or related problems ().
Why should you care?
Retention can trigger urinary tract infections (UTIs), bladder stones, and sleepless nights. It also chips away at confidenceno one likes feeling like they cant finish a bathroom visit.
Why It Happens
Neurogenic bladder and dopamine
Parkinsons robs the brain of dopamine, a chemical that helps coordinate the detrusor muscle (which pushes urine out) and the external sphincter (which holds urine in). Without that smooth signaling, the bladder can become lazy or the sphincter can stay too tight, leading to retention. The disruption of the brainspinalbladder reflex loop explains much of this change.
Nonobstructive vs. obstructive retention
Most Parkinsonrelated cases are nonobstructivethe problem isnt a physical blockage but a signaling glitch. Obstructive retention (like prostate enlargement) can coexist, but its less common in the Parkinsons population.
The nighttime factor
Nighttime bladder control (nocturia) often gets worse as the disease progresses. Lower dopamine levels at night mean the bladder's stop signal is weaker, prompting frequent trips to the bathroom.
Age and disease stage
Higher Hoehn & Yahr stages (the scale doctors use to gauge Parkinsons progression) usually bring more severe urinary issues. In simple terms: the later the stage, the higher the risk.
Recognizing The Signs
Redflag symptoms
- Difficulty starting the stream
- Weak or dribbling stream
- Feeling of fullness even after youve peed
- Need to go multiple times at night (nocturia)
- Sudden, foulsmelling urine (often a sign of infection)
Quick selfassessment checklist
Mark yes if you experience any of these in the past month:
- Do you wake up three or more times to pee?
- Do you feel you cant fully empty your bladder?
- Is your urine odor unusually strong?
- Have you had a fever or pain while urinating?
- Do you need to strain or push to start urination?
Story time
John, 68, thought his busy bathroom schedule was just a sideeffect of his medications. He kept waking up fourfive times each night, feeling exhausted. After a simple bladder scan showed a PVR of 210mL, his neurologist adjusted his meds and added a lowdose mirabegron. Within weeks, his nighttime trips dropped to one or two, and the constant pressure in his lower abdomen faded.
How Doctors Diagnose
Medical history and questionnaires
Doctors start with a detailed symptom diaryoften a standardized Parkinsons bladder questionnaire that captures frequency, urgency, and any leakage.
Physical and neurological exam
Theyll check prostate health (for men), assess muscle tone, and test reflexes that influence bladder control.
Objective tests
- Postvoid residual ultrasound: A painless scan that tells how much urine is left.
- Urodynamics: Measures pressure and flow; used when symptoms are severe or unclear.
- Cystoscopy: Tiny camera inside the bladder, only if a blockage is suspected.
Lab work
A routine urinalysis and culture can rule out infection, while blood glucose checks help exclude diabetic bladder issues.
Expert tip
According to a movementdisorder neurologist at the Cleveland Clinic, If the PVR is consistently above 150mL, or the patient has recurrent UTIs, a referral to a urologist is warranted right away.
Effective Treatment Options
Medication basics
There are two main drug families:
- Anticholinergics (e.g., oxybutynin): Calm an overactive bladder but can cloud memorycaution for older adults.
- 3 agonists (e.g., mirabegron): Relax the bladder muscle without the cognitive sideeffects. Many clinicians now favor mirabegron as a firstline option for Parkinsons patients.
Adjusting Parkinsons meds
Sometimes the culprit is a dopaminergic medication thats too high or too low. Tweaking the dose or switching to a different formulation can ease bladder symptoms without sacrificing motor control.
Catheterisation (when needed)
If you truly cant void, intermittent selfcatheterisation (a clean catheter inserted a few times a day) is often safer than a permanent Foley catheter. Follow a strict hygiene routine to keep infections at bay.
Behavioral and lifestyle hacks
- Timed voiding: Set a schedule (every 23 hours) even if you dont feel the urge.
- Fluid management: Cut caffeine and alcohol in the evening; aim for 1.52L of water spread throughout the day.
- Pelvic floor exercises: Kegels arent just for womenstrengthening the pelvic muscles can improve coordination.
Procedural options
For stubborn cases, doctors may consider:
- Sacral neuromodulation: A tiny device sends gentle electrical pulses to the nerves that control the bladder.
- Botox injections: Temporarily relax the detrusor muscle, reducing urgency and retention.
Emerging therapies
A 2024 clinical trial explored a novel dopaminergic agent (PR001) targeting bladder pathways directly. Early results show a modest reduction in PVR without worsening motor symptoms. Keep an eye on upcoming researchtheres always hope for better options.
Expert insight box
When treating Parkinsons urinary retention, I always start with lifestyle changes, then add mirabegron if needed. Anticholinergics are a last resort because of their impact on cognition, says Dr. Laura Martinez, urologist at Stanford Health Care.
Nighttime Symptom Relief
Why nocturia spikes
Nighttime dopamine dips, combined with reduced bladder capacity, mean the organ cries out for relief more often. Add a full bladder from daytime fluid intake, and youre up at 2 a.m. again.
Targeted nocturia treatments
- Desmopressin (low dose): Lowers urine production at nightuse only if blood sodium is normal.
- Bedtime fluid restriction: Stop drinking two hours before sleep.
- Timed nighttime voiding: If youre a chronic midnight peeper, set an alarm to go once at a convenient hour, then try to sleep through the rest.
Sleepfriendly habits
Place a nightlight in the hallway, keep a small commode or portable urinal by the bed, and wear easytoremove pajamas. Small tweaks can shave minutes off each trip, and those saved minutes add up to a full night of rest.
Realworld example
Maria, 72, used to set three alarms each night. After switching to mirabegron and limiting evening fluids, she now wakes only once, and the trip takes less than a minute. She says, I finally feel like Ive got my evenings back.
Bowel and Bladder Connection
Bowel incontinence and Parkinsons
About 30% of Parkinsons patients also wrestle with constipation or bowel incontinence. The same autonomic nerves that control the bladder also govern the bowels, so problems often travel together.
How constipation worsens retention
A backedup colon can press on the bladder, reducing its ability to empty. Think of it as a traffic jamif the road (colon) is clogged, the cars (urine) cant move smoothly.
Combined management plan
- Highfiber diet: Aim for 2530g of fiber daily (fruits, veggies, whole grains).
- Stool softeners: Polyethylene glycol (Miralax) is a gentle, widely used option.
- Timed bowel program: Same principle as timed voidingschedule a bathroom visit after meals.
- Hydration balance: Enough water to keep stools soft, but not so much that the bladder overfills.
Resource tip
The Parkinsons Foundation offers a free BladderBowel Guide that walks you through daily routines, diet tweaks, and medication reviews ().
Your Practical Checklist
Daily bladder log
Record the time you go, how much you think you void, urgency level (15), and any leaks. Patterns emerge quicklythis log becomes your secret weapon when you visit the doctor.
Medication review
Write down every drug you take, including overthecounter meds and supplements. Note sideeffects like dry mouth or drowsiness, which can clue your physician into why you might be retaining urine.
When to call a doctor
- Fever, chills, or painful urinationpossible UTI.
- PVR consistently >150mL.
- Inability to urinate at all for >24 hours.
- Recurrent nighttime trips (3 per night) despite fluid control.
Preparing for appointments
Bring your bladder log, medication list, and a list of questions (e.g., Is mirabegron safe with my current Parkinsons meds?). Having everything on hand makes the visit efficient and shows youre an engaged partner in your care.
Conclusion
Urinary retention is a common, often hidden sideeffect of Parkinsons disease, driven by the neurogenic bladder changes that affect up to 40% of patients. The good news? Early detection, a balanced mix of medication, lifestyle tweaks, and regular checkins with your health team can keep the problem from spiraling into infections, sleepless nights, and loss of confidence.
Take the first step today: start a simple bladder log, talk openly with your neurologist or urologist, and try one small habit changelike limiting evening caffeine. Youll be surprised how quickly those small moves add up to big relief.
If youve experienced any of these symptoms or have tips that helped you, share them in the comments. Your story could be the lifeline another reader needs. And remember, youre not alonetheres a whole community and a team of specialists ready to support you.
For more on recognizing specific Parkinson bladder control problems and practical management tips, see this helpful guide on Parkinson bladder control.
FAQs
What causes urinary retention in Parkinson’s disease?
Urinary retention in Parkinson’s is mainly due to neurogenic bladder, where disrupted brain-bladder signals prevent the bladder from emptying fully.
How is Parkinson’s urinary retention diagnosed?
Doctors use symptom logs, post-void residual scans, and sometimes urodynamics to measure how much urine remains after urination.
Can medications for Parkinson’s make urinary retention worse?
Yes, some Parkinson’s drugs and anticholinergics can worsen retention; adjusting doses or switching medications may help.
What are the best treatments for urinary retention in Parkinson’s?
Treatments include lifestyle changes, medications like mirabegron, timed voiding, and in severe cases, intermittent catheterization or Botox injections.
When should someone with Parkinson’s seek help for urinary retention?
Seek medical help if you consistently can’t empty your bladder, have pain, fever, or urinate less than normal for over 24 hours.