Hey there, friend. If youre reading this, you (or someone you love) are probably facing the scary phrase recurrent cervical cancer. I know it feels like youve been handed a whole new puzzle, and youre wondering where to start. Good news: there are several proven pathways for recurrent cervical cancer treatment, and understanding them can help you feel a bit more in control. Lets walk through what recurrence means, the main treatment routes, and what you can realistically expect for life expectancy and quality of life.
What Is Recurrence?
Simply put, recurrence means the cancer has come back after it was thought to be gone. It can happen months or even years after the original therapysometimes after a straightup hysterectomy or after radiation. The most common include unexpected bleeding, pelvic pain, a new lump, or changes in urinary or bowel habits. If any of these show up, its worth getting checked right away.
How Doctors Spot a Recurrence
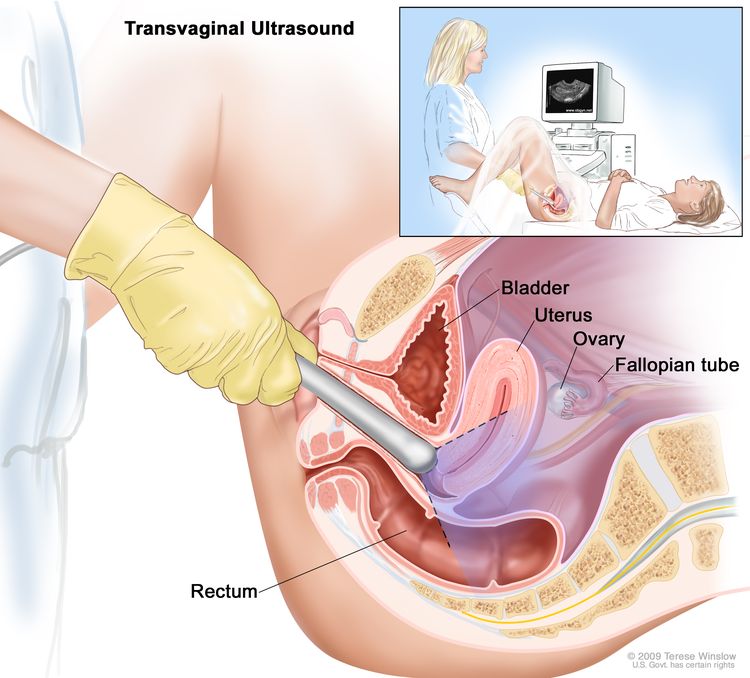
Doctors rely on a mix of imaging (CT, MRI, PET scans), blood tests for tumor markers, and a physical exam. The goal is to pinpoint where the cancer has resurfacedwhether its confined to the pelvis or has spread to distant sites like the lungs or liver.
Treatment Goals Explained
When you hear treatment, you might picture a single, onesizefitsall plan. In reality, there are three main intents: curative (trying to eradicate the disease), diseasecontrol (slowing progression), and palliative (relieving symptoms). Knowing which goal fits your situation helps you weigh the benefits against the risks.
Curative vs. Palliative: When Is Each Realistic?
If the recurrence is limited to the pelvis and you havent reached the maximum safe dose of radiation, a curative approachoften a combo of chemo and radiationmight be on the table. Once the disease has spread widely, the focus often shifts to disease control and symptom relief, using systemic chemotherapy, immunotherapy, or targeted agents.
Balancing Benefits & Risks
Every treatment has sideeffects. Chemoradiation can cause nausea, fatigue, and bladder irritation, while surgery (like pelvic exenteration) carries the risk of major complications and a long recovery. The key is to match the treatments potential to extend life or improve its quality with what youre willing and able to handle.
Standard Treatment Options
| Modality | Typical Regimen | When Used | Key Benefits | Main Risks |
|---|---|---|---|---|
| Chemoradiation | Cisplatin+5FUMitomycin + pelvic RT | Pelviconly recurrence after hysterectomy | High local control, potential cure | Acute GI/urinary toxicity, fatigue |
| Surgery (Pelvic Exenteration) | Radical removal of pelvic organs | Isolated central recurrence, no distant disease | Potential cure in very select cases | Major morbidity, lengthy rehab |
| Systemic Chemotherapy | Carboplatin+Paclitaxel, Topotecan, etc. | Distant/metastatic recurrence | Controls spread throughout the body | Myelosuppression, neuropathy |
| Immunotherapy | Pembrolizumab (PD1 inhibitor) chemo | PDL1positive tumors after chemo failure | Durable responses for some patients | Immunerelated sideeffects (skin, GI, endocrine) |
| Targeted / ADCs | Tisotumab vedotin (FDAapproved) | 2nd/3rdline after chemo | Higher response rates vs. chemo alone | Infusion reactions, ocular toxicity |
How Chemoradiation Works
Cisplatin acts as a radiosensitizerit makes cancer cells more vulnerable to radiation. This combo has been the backbone of curative intent for many years according to multiple trials.
When Surgery Is an Option
Pelvic exenteration is a massive operation, but in carefully selected patients with a single central recurrence, cure rates can reach 3040%. The decision hinges on prior radiation dose, overall health, and personal goals.
Emerging Systemic Options
Immunotherapy (like pembrolizumab) and antibodydrug conjugates such as tisotumab vedotin are expanding the toolbox, especially for patients whose cancer has become resistant to standard chemo. These newer agents can offer longer disease control with a different sideeffect profile.
Tailoring Treatment Choices
| Clinical Factor | Preferred Modality | Rationale |
|---|---|---|
| Recurrence < 2years after hysterectomy | Chemoradiation or exenteration | Aggressive biology; early relapse needs strong local control |
| Prior fulldose pelvic radiation | Systemic chemo / immunotherapy | Radiation dose limits prevent safe reirradiation |
| Stage1b2 primary cancer now recurrent | Consider surgery if isolated | Higher chance of cure with complete removal |
| Metastatic spread (lung, liver) | Systemic chemo immunotherapy | Treats disease throughout the body |
What If Ive Already Had Radiation?
When the pelvis has already received the maximum safe dose, doctors often turn to systemic optionschemo, immunotherapy, or a clinical trial that offers a novel agent. Reirradiation is sometimes possible with highly focused techniques, but its the exception rather than the rule.
Can I Combine Immunotherapy With Chemo?
Yes! Recent studies show that adding pembrolizumab to standard chemotherapy improves overall survival for many patients to the KEYNOTE826 trial. Your oncology team will weigh the benefits against potential immunerelated sideeffects.
Managing Side Effects
Every treatment comes with a sideeffect checklist, but the good news is that most can be mitigated with proactive care.
Acute Toxicities
- Nausea & vomiting: Antiemetics like ondansetron work wonders.
- Fatigue: Gentle walks and short naps help keep energy levels stable.
- Diarrhea or constipation: Overthecounter loperamide or fiber supplements, under doctor guidance.
LongTerm Concerns
Pelvic fibrosis, sexual health changes, and urinary irritation can linger after radiation. Pelvic floor physical therapy, counseling, and specialized urology referrals can improve quality of life.
Life Expectancy Insights
Life expectancy for recurrent cervical cancer varies widely. Median overall survival after curativeintent chemoradiation is about 1224months, while newer immunotherapy regimens are pushing some patients beyond the twoyear mark. Factors that tilt the odds in your favor include early detection of recurrence, good performance status, and access to clinical trials. For men facing prostate cancer, understanding prostate removal life expectancy can also offer insights into managing expectations and treatment planning.
RealWorld Patient Stories
Stories resonate because they turn statistics into lived experience. Here are a couple of brief snapshots (with permission):
Marias Journey After 2Years
Maria was declared cancerfree after a hysterectomy and radiation. Two years later, she felt a pressure in her lower abdomen. A PET scan revealed a small pelvic recurrence. Her team chose chemoradiation combined with pembrolizumab. Today, 18months later, shes back to gardening and says the sideeffects were manageable with the right support.
Jennas Path After Hysterectomy
Jenna had a hysterectomy with no radiation initially. When her cancer returned, the doctors recommended pelvic exenterationa daunting operation. She decided against surgery and went on systemic chemotherapy followed by a clinical trial drug. She now volunteers to help others navigate the emotional rollercoaster of decisionmaking.
Both narratives highlight how personal values, disease specifics, and treatment sideeffects intertwine to shape the best path for each individual.
Common Questions Answered
What Is the Most Common Recurrent Cervical Cancer Treatment?
Globally, chemoradiationcisplatinbased chemotherapy given with pelvic radiationremains the frontline option for most localized recurrences.
Can Recurrence Be Cured?
In select cases where the tumor is confined and the patient is in good health, cure is possible, especially with combined surgery and radiation. More often, treatment aims to control disease and preserve quality of life.
How Long Is Life Expectancy After Recurrence?
Median survival ranges from 12 to 24months, but newer therapies are extending outcomes for a subset of patients. Individual prognosis depends on stage, biology, and response to treatment.
Is Surgery Still an Option After Radiation?
Only if the previous radiation dose was low enough to allow safe reirradiation or if the recurrence is surgically resectable without exceeding tissue tolerance.
What Are the Main SideEffects of Chemoradiation?
Typical acute effects include nausea, fatigue, bladder irritation, and bowel changes. Most are temporary and can be managed with medication and supportive care. If you are also managing prostate cancer, advances in early prostate cancer treatment may provide additional options.
When to Seek Help
If you notice any of the following redflag signs, call your oncology team right away:
- Heavy or abnormal vaginal bleeding
- Severe pelvic pain that doesnt improve with usual meds
- New lumps or swelling in the abdomen or pelvis
- Sudden changes in urinary or bowel habits
Quick action can catch a recurrence at an earlier, more treatable stage.
Final Thoughts & Steps
Facing a recurrence feels like being asked to climb a steep hill in the dark. But youre not alonedoctors, support groups, and friends like me are here to shine a light. Remember:
- Know your treatment goalscurative, control, or comfort.
- Ask about all options, including clinical trials and newer immunotherapies.
- Monitor symptoms closely and seek help early.
- Lean on your support network; sharing experiences can lighten the emotional load.
If you have questions or want to share your own story, drop a comment below. Your voice might be the encouragement someone else needs. Together, we can navigate this journey with knowledge, hope, and a little bit of courage.
FAQs
What are the most common treatment options for recurrent cervical cancer?
Typical choices include chemoradiation, pelvic exenteration surgery, systemic chemotherapy, immunotherapy (e.g., pembrolizumab), and targeted agents such as antibody‑drug conjugates.
Can recurrent cervical cancer be cured?
Cure is possible in highly selected cases where the disease is isolated to the pelvis and the patient has good performance status; otherwise, treatment aims to control disease and maintain quality of life.
How does immunotherapy work for recurrent cervical cancer?
Immunotherapy drugs block the PD‑1/PD‑L1 pathway, allowing the immune system to recognize and attack cancer cells, and have shown durable responses in PD‑L1‑positive tumors.
What side effects should I expect from chemoradiation?
Common acute effects are nausea, fatigue, bladder irritation, and bowel changes; most are manageable with medication and supportive care, while long‑term effects may include pelvic fibrosis and sexual health changes.
When should I contact my doctor about possible recurrence?
Reach out promptly if you notice heavy or abnormal bleeding, new pelvic pain, unexplained lumps, or sudden changes in urinary or bowel habits.