At a Glance
Bottomline answer
If your joints puff up as a whole digit after a recent stomach or genital infection, youre probably dealing with reactive arthritis. If the swelling is isolated to individual joints, appears on both sides of your body, and you have positive rheumatoid factor (RF) or antiCCP antibodies, rheumatoid arthritis (RA) is the likely diagnosis.
Quick checklist for readers
- Recent infection (GI or GU)? Think reactive.
- Symmetrical joint pattern? Think RA.
- Extraarticular signs (eye redness, skin rash)? Reactive.
- Blood test positive for RF/antiCCP? RA.
When youre staring at a swollen toe, this quick list can save you a lot of whatif brainfog. And remember the only way to be sure is to see a rheumatologist.
How They Start
Reactive arthritis: the infectiontriggered cascade
Reactive arthritis usually follows an infection that originates in the gut, urinary tract, or genital area. Common culprits include Chlamydia trachomatis, Salmonella, Shigella, Yersinia, and Campylobacter. After you clear the infection, your immune system sometimes goes into overdrive, targeting your joints instead of the bug. This misdirected response typically appears 14 weeks after the initial illness.
Rheumatoid arthritis: autoimmune origins
RA isnt sparked by an infection; its an autoimmune disease where your body mistakenly attacks its own joint lining. Genetics (especially the HLADRB1 shared epitope), smoking, and being female (women are about three times more likely to develop it) are the biggest risk factors. The exact trigger is still a research puzzle, but the bodys own immune cells become the aggressors.
Sidebyside comparison
| Aspect | Reactive Arthritis | Rheumatoid Arthritis |
|---|---|---|
| Typical trigger | Recent bacterial infection (GI or GU) | Autoimmune, no clear infection |
| Onset age | 2040years | 3060years |
| Gender bias | Slight male predominance | Female predominance (3:1) |
| Genetic marker | HLAB27 (50% positive) | HLADRB1 shared epitope |
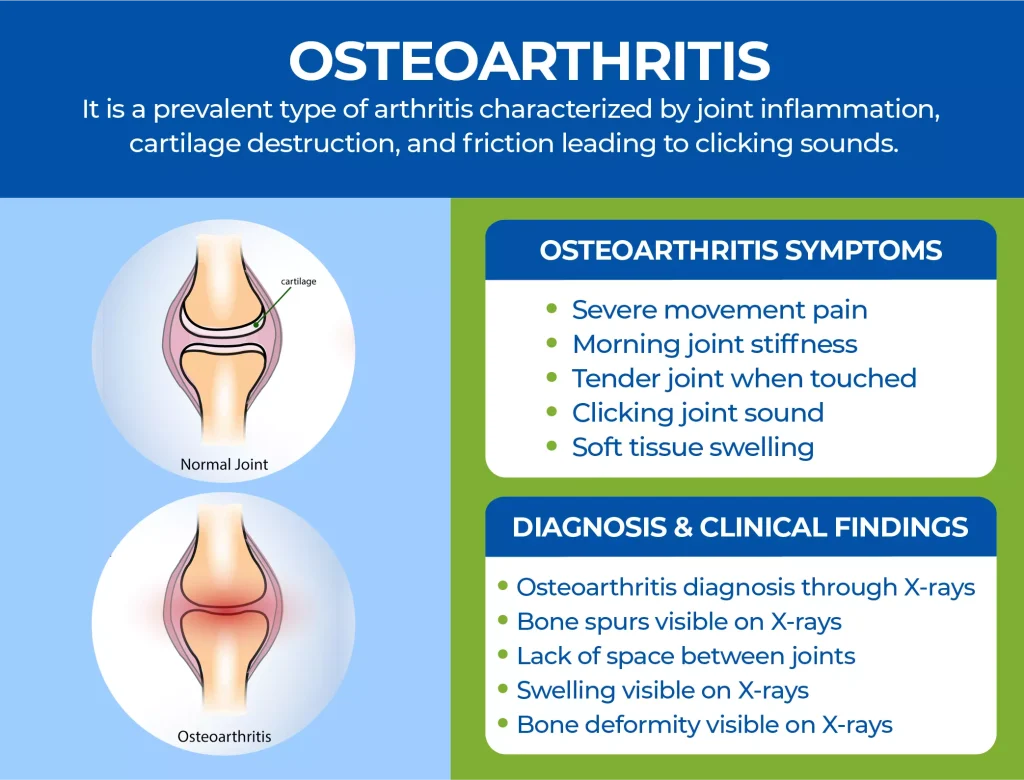
Symptoms That Differ
Jointspecific patterns
With reactive arthritis, the swelling often involves an entire finger or toe, giving it a sausage appearance (medically called dactylitis). The pain tends to be asymmetricone hand or foot may feel worse than the other. You might also notice enthesitis, which is tenderness where tendons attach to bone, especially around the heels.
Rheumatoid arthritis, on the other hand, loves symmetry. It typically hits the same joints on both sidesthink both wrists, both knees, or both knuckles. Morning stiffness that lasts longer than 30minutes is a classic red flag, and you may develop rheumatoid noduleslittle, firm bumps under the skin.
Systemic signs
Reactive arthritis doesnt stay confined to the joints. Around a third of patients develop conjunctivitis (red, watery eyes), urethritis (painful pee), or skin lesions called keratoderma blennorrhagicum. These extraarticular clues can steer doctors toward a postinfectious diagnosis.
RA is a systemic disease, too, but its extras usually involve fatigue, lowgrade fever, and anemia of chronic disease. Some patients also report a vague flulike feeling before the joint pain really kicks in.
Quickreference chart
| Feature | Reactive Arthritis | Rheumatoid Arthritis |
|---|---|---|
| Joint pattern | Asymmetric, dactylitis | Symmetric polyarthritis |
| Morning stiffness | Usually <30min | >30min, often >1hour |
| Eye involvement | Common (conjunctivitis) | Rare |
| Blood test markers | RF/antiCCP negative, HLAB27 +/- | RF/antiCCP positive |
Diagnosis and Pitfalls
Laboratory workup
For reactive arthritis, doctors usually see a normal or only mildly elevated ESR/CRP, and the rheumatoid factor and antiCCP antibodies come back negative. A positive HLAB27 test can support the diagnosis, but its not mandatory.
In rheumatoid arthritis, the lab picture is more dramatic. Elevated ESR and CRP signal inflammation, while RF and antiCCP antibodies are often positiveespecially antiCCP, which is highly specific for RA.
Imaging clues
Xrays in early RA reveal joint space narrowing and erosionstiny punchedout bits of bone that signal aggressive disease. Reactive arthritis may look completely normal on Xray at first; later on, you might see enthesophytes (bone spurs where tendons attach) if the inflammation lingers.
Advanced imaging like MRI or ultrasound can detect synovitis (joint lining inflammation) before any bone damage appearsa handy tool when the clinical picture is muddled.
Common misdiagnoses
Its easy for doctors to mistake RA for other inflammatory arthritides. Psoriatic arthritis, ankylosing spondylitis, lupus, Lyme disease, and even gout can produce similar joint pain. A rare but notable confusion is with multiple sclerosis (MS), which primarily causes neurological symptoms rather than joint swelling; however, neuropathic pain from MS can be misinterpreted as joint pain in a hurried evaluation.
Decisiontree flowchart (text version)
Step1: Recent infection? Yes Consider reactive arthritis.
Step2: Symmetrical joint swelling? Yes Consider RA.
Step3: RF/antiCCP positive? Yes RA likely.
Step4: HLAB27 positive+extraarticular signs? Supports reactive.
Step5: Imaging findings? Erosions RA; enthesophytes reactive.
Treatment Options Overview
Reactive arthritis
Firstline therapy is usually a nonsteroidal antiinflammatory drug (NSAID) like ibuprofen or naproxen. If your reactive arthritis is tied to a bacterial infectionsay, chlamydiayour doctor will add a targeted antibiotic (doxycycline is a common choice). Most people feel better within a few weeks.
When symptoms stick around for more than six months, some rheumatologists introduce diseasemodifying antirheumatic drugs (DMARDs) such as sulfasalazine or methotrexate. These arent always necessary, but they can calm persistent inflammation.
Rheumatoid arthritis
RA demands early, aggressive treatment to prevent joint erosion. The cornerstone is a DMARDusually methotrexatestarted as soon as the diagnosis is confirmed. If disease activity remains high, doctors may add biologic agents (TNF inhibitors, IL6 blockers) or newer JAK inhibitors.
The modern treattotarget approach, championed by the , aims for remission or low disease activity within six months. Frequent monitoring of blood counts and liver function is essential because these meds can have side effects.
Shared concerns
Both conditions involve medication that can thin the blood, upset your stomach, or increase infection risk. If youre planning a pregnancy, talk to your doctor earlysome drugs are safe, others arent. Lifestyle tweaks (regular gentle exercise, balanced diet, smoking cessation) boost the effectiveness of any treatment plan.
ProsCons table
| Aspect | Reactive Arthritis | Rheumatoid Arthritis |
|---|---|---|
| Typical duration | Often selflimited (612months) | Chronic, lifelong management |
| Firstline meds | NSAIDs antibiotics | DMARDs (methotrexate) biologics |
| Risk of joint damage | Low to moderate | High without early treatment |
| Systemic symptoms | Eye, skin, urinary involvement | Fatigue, anemia, lung involvement |
Key Takeaways for You
Understanding whether youre facing reactive arthritis or rheumatoid arthritis isnt just academicit directly shapes the labs your doctor orders, the medications youll take, and the longterm outlook for your joints. Reactive arthritis usually follows a gut or genital infection, shows up as sausage swelling, and may resolve on its own or with shortterm NSAIDs and antibiotics. Rheumatoid arthritis is a systemic autoimmune disease that thrives on early, aggressive DMARD therapy to keep joints from eroding.
If any of the redflag signs described above feel familiarespecially recent infection, asymmetric swelling, or persistent morning stiffnessdont wait. Grab a notebook, jot down your symptoms, and book an appointment with a rheumatologist. Bring this checklist along; it will help the specialist zero in on the right diagnosis faster.
Weve covered triggers, symptoms, diagnostic tricks, and treatment pathways, but the most important step is you taking action. Your joints deserve a clear answer, and you deserve care thats backed by science and compassion. Have questions? Share your story in the comments, and lets keep the conversation going. Together we can turn confusion into confidence.
For guidance on longerterm management and criteria used to define remission, many patients and clinicians refer to established targets such as AS remission criteria when assessing treatment success and planning followup.
FAQs
What is the main cause of reactive arthritis?
Reactive arthritis is usually triggered by a recent bacterial infection of the gastrointestinal or genitourinary tract, such as Chlamydia, Salmonella, or Shigella.
How can I tell if my joint pain is rheumatoid arthritis?
Rheumatoid arthritis typically causes symmetric joint swelling, prolonged morning stiffness (over 30 minutes), and positive blood tests for rheumatoid factor (RF) or anti‑CCP antibodies.
Is there a cure for reactive arthritis?
There is no permanent cure, but most cases improve with NSAIDs, targeted antibiotics (if a bacterial cause is identified), and, when needed, short‑term DMARDs.
Why are extra‑articular symptoms important in diagnosis?
Features like conjunctivitis, urethritis, or skin lesions point toward reactive arthritis, whereas systemic signs such as fatigue, anemia, and lung involvement are more typical of rheumatoid arthritis.
What are the first‑line treatments for rheumatoid arthritis?
The cornerstone is early use of disease‑modifying antirheumatic drugs (DMARDs) such as methotrexate, often combined with NSAIDs and, if needed, biologic agents to achieve remission.