Quick answer:RA remission is a state where disease activity is so low that you barely notice any joint pain, swelling, or morning stiffness. Clinicians decide this by using the ACR/EULAR2022 core set, DAS28, SDAI, CDAI, or the newer Boolean2.0 rulesand they usually want you to meet the numbers for at least two straight months.
Why you should keep reading:Well break down exactly what those numbers mean, how long remission can actually last, whether you can stay off meds, realworld stories from people just like you, and lifestyle hacks (diet, exercise, stressbusting) that help keep the flare away. Grab a cup of tea, and lets dive in.
Official Remission Criteria
What does the ACR/EULAR 2022 core set include?
The American College of Rheumatology and the European Alliance of Associations for Rheumatology (ACR/EULAR) agreed on six simple variables. If you meet at least five of those for two consecutive months, youre officially in remission:
- Morning stiffness <15minutes
- No fatigue
- No joint pain
- No tender joints
- No swollen joints
- CRP<1mg/dL or ESR<30mm/h (women) /<20mm/h (men)
These are the quickcheck items doctors use during a routine visit. Its a neat way to capture the whole picture without a mountain of tests.
How is disease activity measured? (DAS28, SDAI, CDAI)
When rheumatologists need a more nuanced look, they turn to validated scores. Below is a handy comparison:
| Score | Threshold for Remission | What It Uses |
|---|---|---|
| DAS28 | <2.6 | Tender/Swollen Joint Count (28 joints), ESR/CRP, Patient Global Assessment |
| SDAI | 3.3 | Tender/Swollen Joint Count (28 joints), Patient & Physician Global, CRP |
| CDAI | 2.8 | Tender/Swollen Joint Count (28 joints), Patient & Physician Global (no lab) |
These scores are interchangeable in practice, but many clinics favor SDAI because it balances patientreported feelings with objective labs.
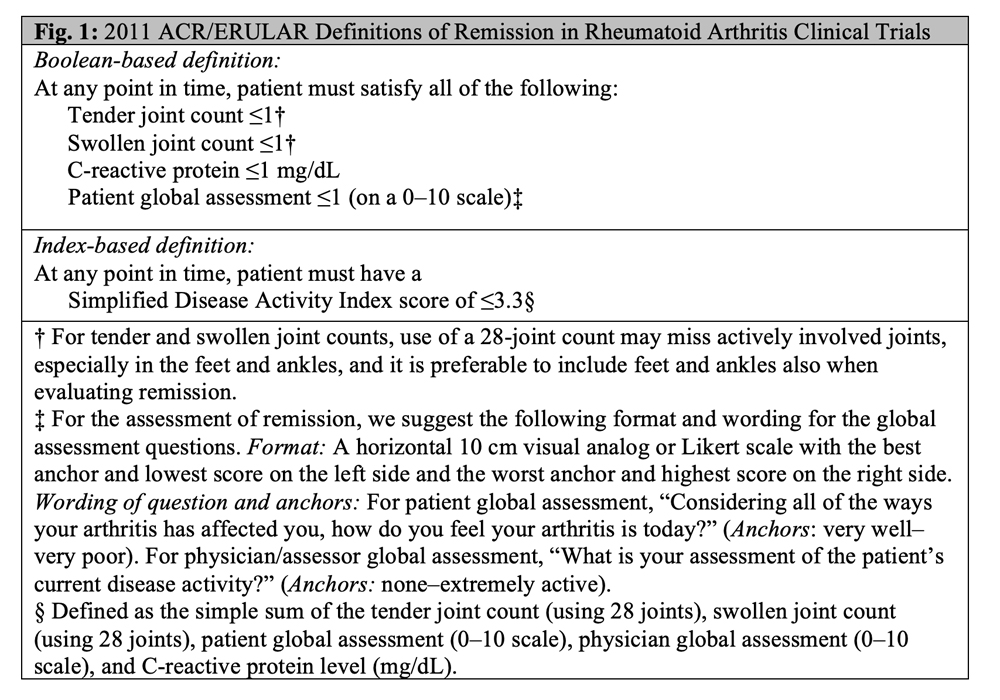
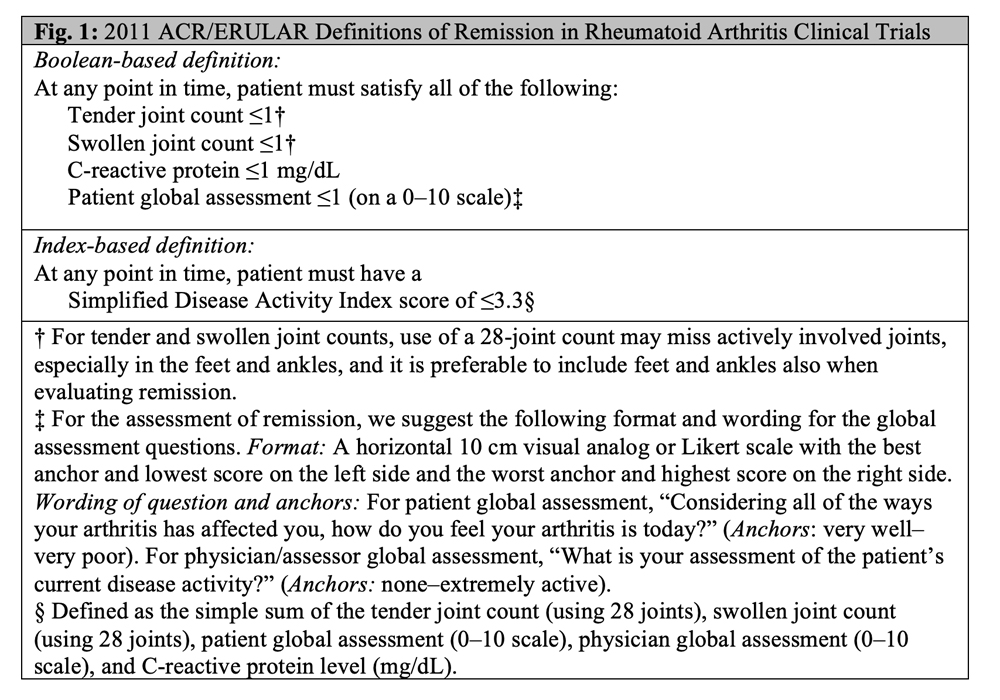
What is the Boolean1.0 vs. Boolean2.0 criteria?
Boolean1.0 is the oldest allornothing rule:
- Tender Joint Count 1
- Swollen Joint Count 1
- CRP 1mg/dL
- Patient Global 1 (010 scale)
It works well but can be too strict, especially for patients who have a tiny uptick in CRP that isnt clinically important. Thats why the research community introduced Boolean2.0 criteria in 2023:
- TJC 1
- SJC 1
- CRP 1mg/dL or ESR 20mm/h
- Patient Global 2
Boolean2.0 captures about 1015% more patients who truly feel in remission while still keeping the bar high enough to avoid false optimism.
How long must the criteria be met?
The guidelines say you need to hit the numbers for at least two consecutive months. In everyday practice, many rheumatologists look for a sustained sixmonth period before calling it stable remission and considering medication tapering.
Expert tip: How rheumatologists apply these criteria in a busy clinic
Dr. Elena Martnez, a boardcertified rheumatologist in Boston, says she uses a simple checklist on the exam room tablet. If the patient already knows the numbers, they often tell me I think Im in remission. That saves us both time, and we can focus on what keeps it that way.
Remission Duration Insights
Typical duration of remission in realworld cohorts
Large registries from the US and Europe show that roughly 3040% of patients stay in remission for at least one year after achieving it. The median durability is about 14months, but theres a wide spreadsome people stay flarefree for 5years, others slip after a few weeks.
Factors that predict longer remission
- Early aggressive therapy: Starting a biologic or JAK inhibitor within the first six months of diagnosis dramatically improves longterm odds.
- Low baseline DAS28: The lower your score when you first start treatment, the easier it is to stay low.
- Seronegative status: Patients without rheumatoid factor (RF) or antiCCP antibodies tend to have milder disease trajectories.
- Adherence: Skipping doses or appointments is the single biggest predictor of a future flare.
- Lifestyle: Regular exercise, a Mediterraneanstyle diet, and good sleep all add small but meaningful buffers. For those interested in joint health, consultation on ankylosing spondylitis remission can provide insight into related inflammatory conditions.
Can remission be permanent?
In short: probably not. RA is a chronic autoimmune condition, and the immune system loves surprises. Even after years of silence, a modest infection, stress, or a missed medication can reignite inflammation.
Case study: Janes 3year medicationfree remission
Jane, a 42yearold graphic designer, shared her story on . After 18months of a TNF inhibitor and methotrexate, her DAS28 dropped to 1.8, and she met the Boolean2.0 criteria for two months straight. Together with her rheumatologist, she tapered the biologic over six months, then stopped methotrexate after another year. Six months later, she switched to a strict Mediterranean diet, added daily 30minute walks, and kept an eye on her ESR every three months. Shes now three years flarefree, attending checkups only twice a year.
Visual aid: Timeline of remission durability
Imagine a line that stretches from 1month to 5years. Most patients cluster around the 12month mark, a smaller group punches through the 3year line, and a tiny handfullike Janekeep the line going beyond five years.
Real Patient Stories
My RA went quiet after 6months of combo therapy
Mike, a 55yearold accountant, posted on a rheumatoid arthritis forum that after six months of a biologic plus lowdose steroids, his SDAI hit 2.5 and stayed there. He says the biggest surprise was how normal his mornings feltno longer a battle with stiffness.
Living medicationfree for 2years
Lena, a mother of two, stopped all diseasemodifying drugs after 24months of sustained remission. She credits a strict routine: 150minutes of moderate exercise per week, daily omega3 capsules, and a nightly habit of journaling stressors and outcomes. Her doctor continues to monitor her labs every six months.
What we can learn from these stories
The recurring themes are clear:
- Early, aggressive treatment followed by steady monitoring.
- Strong partnership with a rheumatologist whos comfortable with tapering.
- Lifestyle choices that keep the immune system calm.
These anecdotes are inspiring, but remember: each body is unique. What works for Mike may need tweaking for you.
Expert commentary: Why anecdotes need clinical validation
Dr. Priya Patel, a senior researcher at the Arthritis Foundation, reminds us that realworld experiences are valuable, but they must be interpreted alongside randomized controlled trials. She encourages patients to bring any personal data (symptom logs, lab results) to their appointments so the doctor can align stories with science.
MedicationFree Remission?
What does the evidence say?
Several trials have examined tapering biologics after sustained remission. A 2021 randomized study found that patients who tapered over 12weeks had a 30% flare rate within a year, compared to 15% when the drug was kept at full dose. Importantly, most flares were mild and responded quickly to restarting therapy.
Risks of stopping therapy early
- Joint damage: Even a short flare can accelerate erosions if not caught early.
- Symptom rebound: Some patients feel an aftershock of pain that lingers for weeks.
- Loss of confidence: Reentering treatment after a flare can feel discouraging.
Guidelines for a safe drug holiday
Professional societies suggest the following when considering a taper:
- Document at least six months of stable remission (using DAS28<2.6 or Boolean2.0).
- Discuss the plan with your rheumatologist; obtain a written taper schedule.
- Reduce the dose graduallyusually 1020% every 23months.
- Schedule labs (CRP/ESR) and joint exams at each step.
- Have a rescue plan: a rapidrestart of the previous dose if any flare signs appear.
Patient checklist before tapering
- Stable DAS28 <2.6 for 6months
- No radiographic progression on recent Xray
- Consistent medication adherence record
- Good sleep quality (7hours/night)
- Low stress levels (validated questionnaire score <5)
- Support system in place (family, therapist, or support group)
- Willingness to monitor symptoms daily for the next 12weeks
Expert input: Treattotarget vs. treattomaintain
Dr. Michael Nguyen explains, Treattotarget means we aim for remission and stay there, adjusting therapy as needed. Treattomaintain is more about keeping you comfortable without necessarily chasing the strict numbers. He advises patients who crave medication freedom to adopt a treattotarget mindset first, then discuss tapering as a secondary goal.
Lifestyle Support Tips
Is there an RA remission diet?
There isnt a magic recipe, but many studies point to the antiinflammatory power of a Mediterraneanstyle eating plan:
- Plenty of oily fish (salmon, sardines) for omega3s.
- Olive oil as the main fat source.
- Colorful vegetables and fruitsespecially berries and leafy greens.
- Whole grains, nuts, and legumes.
- Limited red meat, processed foods, and added sugars.
A 2020 systematic review found that patients who adhered to this diet had a modest but statistically significant reduction in DAS28 scores.
Exercise recommendations
Movement is medicine. Aim for a balanced routine:
- Lowimpact cardio: Walking, swimming, or cycling 150minutes per week.
- Strength training: Light weights or resistance bands 23 times a week to protect joints. For guidance on appropriate exercises especially for bone and joint health optimization, see osteoporosis exercises.
- Flexibility & balance: Yoga or tai chi 2 times weeklygreat for morning stiffness.
Start slow; even a 10minute daily walk can shave minutes off morning stiffness over time.
Stress & sleep
Stress hormones can ignite inflammation. Simple practicesdeepbreathing, meditation, or a 5minute gratitude journallower cortisol. Sleep matters too; aim for 78hours of uninterrupted rest. If you struggle, try a techfree winddown routine an hour before bed.
Supplements with evidence
While not replacements for prescription meds, a few supplements have modest data:
- Fish oil (EPA1g/day)
- Vitamin D (8001,000IU/day if deficient)
- Curcumin (standardized extract 5001,000mg/day)
Always talk to your rheumatologist before adding themespecially if youre on blood thinners.
Quickreference table: What to add vs. what to avoid
| Add | Avoid |
|---|---|
| Olive oil, fatty fish, nuts | Processed meats, sugary drinks |
| Leafy greens, berries, whole grains | Refined carbs, excess alcohol |
| Daily lowimpact exercise | Sedentary lifestyle |
Practical Remission Checklist
Step1: Confirm criteria
Use either DAS28<2.6, SDAI3.3, CDAI2.8, or Boolean2.0. Make sure the numbers hold steady for at least two months.
Step2: Baseline labs & imaging
Order ESR/CRP, CBC, and a recent Xray. No new erosions? Youre in good shape.
Step3: Shared decision on medication
Discuss with your rheumatologist whether a slow taper or continued lowdose maintenance best matches your life goals.
Step4: Lifestyle lockin
Commit to the Mediterranean diet, 150minutes of cardio per week, and a nightly sleep routine.
Step5: Monitoring schedule
Plan rheumatology visits every three months for the first year of tapering, then every six months if you stay flarefree.
Downloadable PDF
Well soon add a printable version of this checklistperfect for keeping on your fridge or in your medical folder.
Conclusion
Understanding the RA remission criteria is the first step toward reclaiming control of your life. Whether youre aiming for a medicationfree future or simply want to keep flares at bay, the numbers (DAS28, SDAI, Boolean2.0) give you a clear map. Remember, remission can last months, years, or even longerbut staying vigilant, partnering with a trusted rheumatologist, and embracing supportive lifestyle habits are the real secret ingredients.
If youve reached remission, congrats! Share your story below or on Reddits RA communityyour experience could be the spark someone else needs. And if youre still hunting for that quiet phase, dont lose hope; the tools are there, and youre not alone on this journey.
FAQs
What are the main components of the ACR/EULAR 2022 RA remission criteria?
The criteria include morning stiffness < 15 minutes, no fatigue, no joint pain, no tender or swollen joints, and a CRP < 1 mg/dL or ESR below gender‑specific thresholds, with at least five of six needed for two consecutive months.
How do DAS28, SDAI, and CDAI differ in defining remission?
DAS28 uses 28‑joint counts, ESR/CRP and patient global assessment with a remission cutoff < 2.6. SDAI adds physician global and CRP, remission ≤ 3.3. CDAI omits labs, using only joint counts and both global scores, remission ≤ 2.8.
What is the advantage of Boolean 2.0 over Boolean 1.0?
Boolean 2.0 relaxes the patient‑global threshold to ≤ 2 and allows ESR ≤ 20 mm/h as an alternative to CRP, catching 10‑15 % more patients who truly feel in remission while keeping criteria strict.
Can I stop my RA medication once I reach remission?
Guidelines suggest a minimum of six months of stable remission before considering a gradual taper, with a clear rescue plan. Sudden stoppage can lead to flares and joint damage.
What lifestyle changes support long‑term RA remission?
Adopting a Mediterranean‑style diet, regular low‑impact cardio, strength training, adequate sleep, stress‑reduction techniques, and evidence‑based supplements like fish oil can help maintain remission.