Imagine you walk into a cardiology clinic feeling unusually winded after climbing just one flight of stairs. The doctor orders a simple ultrasound a transthoracic echo and within minutes you have a snapshot of the pressure inside your lungs arteries. That snapshot, when read with the right echo criteria, can tell you whether youve got mild, moderate, or severe pulmonary hypertension (PH) and, more importantly, whether you need further testing right away.
In the next few minutes well walk through exactly how those echo numbers are measured, what they mean, and how you (or your loved one) can use them to stay ahead of this serious condition. No dense textbooks, just plaintalk, friendly guidance, and a few handy tables you can print out for the next appointment.
What is Echo?
Echo is short for echocardiogram an ultrasound of the heart that uses sound waves to create moving pictures of your hearts chambers, valves, and blood flow. Its the goto screening tool for pulmonary hypertension because its quick, painless, and gives doctors a look at the pressure the right side of the heart is working against.
How does echo estimate pulmonary pressure?
The echo doesnt measure pressure directly. Instead, it looks at how fast blood is moving through the tricuspid valve (theTRvelocity) and uses a simple formula that adds an estimate of rightatrial pressure (RAP). The result is an estimate of the pulmonary artery systolic pressure (PASP), which is a good surrogate for the mean pulmonary artery pressure used in rightheart catheterization.
Why rely on echo first?
Rightheart catheterization is the gold standard, but its invasive. Echo gives a rapid, noninvasive screen that can flag patients who need that deeper dive. In many clinics, a normal echo can spare a patient an unnecessary procedure.
Core Echo Measurements
| Measurement | What It Shows | Typical Cutoff | Clinical Meaning |
|---|---|---|---|
| TRVelocity (TRV) | Peak systolic speed of blood through tricuspid valve | >3.4m/s highprobability PH | Higher velocity = higher RVSP |
| RightVentricular Systolic Pressure (RVSP) | Estimated pressure in right ventricle | 45mmHg moderatetosevere | Often reported as RVSP=mmHg |
| Pulmonary Artery Systolic Pressure (PASP) | RVSP minus RAP | >35mmHg suspicion of PH | Direct echo surrogate for pulmonary pressure |
| Pulmonary Artery Acceleration Time (PAAT) | Time from onset to peak flow in PA | <105ms elevated PAP | Useful when TR jet is poor |
| IVC Size & Collapsibility | Estimates RAP | Diameter >2.1cm with <50% collapse RAP15mmHg | Feeds into PASP calculation |
Measuring TR Velocity correctly
Grab the continuouswave Doppler cursor and line it up with the direction of blood flow through the tricuspid valve. A slight offaxis angle can underestimate the velocity think of trying to listen to a conversation from the back of a crowded room; youll miss some of the nuances.
Estimating RAP from the IVC
Look at the inferior vena cava (IVC) in the subcostal view. If the IVC is wide (>2.1cm) and barely collapses when the patient inhales sharply (sniff test), you assign an RAP of about 15mmHg. If its narrow and collapses >50%, you use 5mmHg. This little step often makes the difference between a borderline and a definite PH diagnosis.
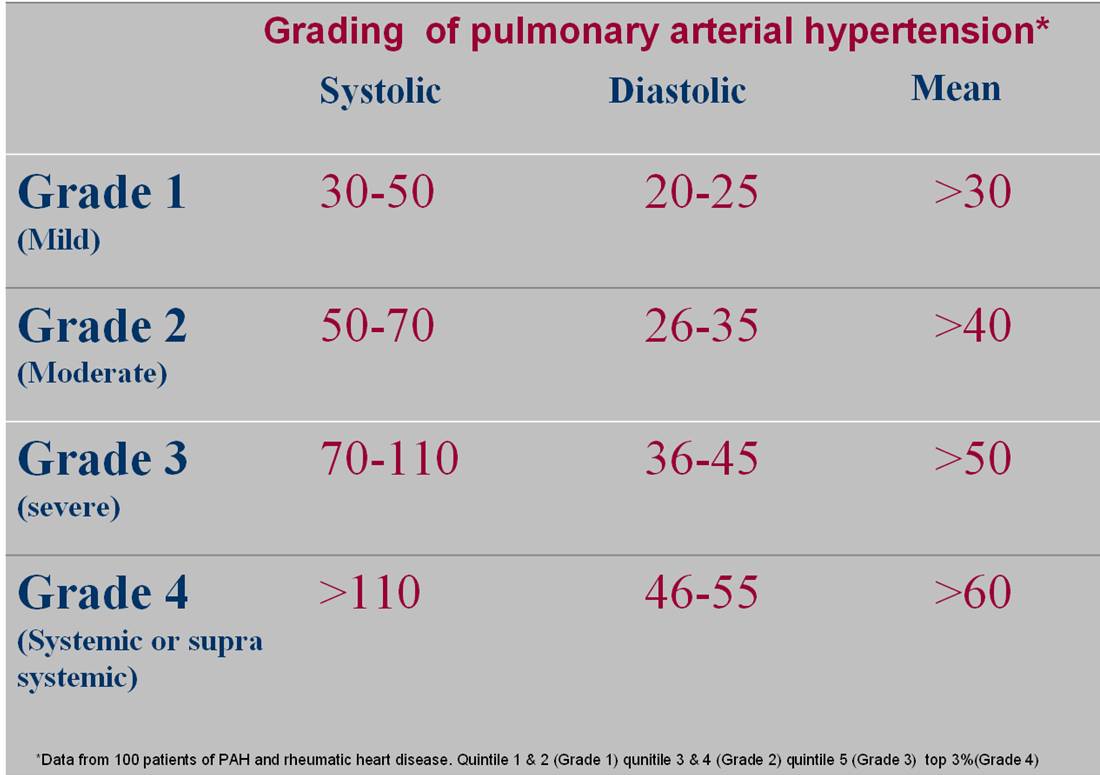
Echo Severity Classification
What counts as mild, moderate, or severe?
Using the numbers from the table, most labs follow a threetier system:
- Mild PH: PASP3040mmHg or TRV2.63.0m/s.
- Moderate PH: PASP4155mmHg or TRV3.03.4m/s.
- Severe PH: PASP>55mmHg or TRV>3.4m/s.
These ranges line up with the for rightheart assessment and give a clear language to talk with your doctor about mild pulmonary hypertension on echo versus moderate or severe.
How does RVSP grading fit?
RVSP is another way to state the same thing: an RVSP of 3045mmHg usually corresponds to mild disease, 4660mmHg to moderate, and >60mmHg to severe. Remember that RVSP includes the estimated RAP, so a high RAP can make the PASP look a little lower than the true pressure.
Echo vs. catheter numbers
Below is a quick sidebyside comparison you can keep on the fridge:
| Echo Estimate | Typical RHC Value | Interpretation |
|---|---|---|
| PASP3040mmHg | Mean PAP2025mmHg | Mild PH |
| PASP4155mmHg | Mean PAP2535mmHg | Moderate PH |
| PASP>55mmHg | Mean PAP>35mmHg | Severe PH |
Measuring Pulmonary Pressure
Stepbystep formula
The classic equation is:
PASP = 4 (TRV) + RAP
Lets break it down with a realworld example. Say your echo shows a TR velocity of 3.2m/s and the IVC suggests an RAP of 10mmHg.
- Square the TRV: 3.2 = 10.24.
- Multiply by 4: 10.24 4 = 40.96.
- Add RAP: 40.96 + 10 51mmHg.
That lands you in the moderatetosevere range, signaling that a rightheart catheter is probably the next step.
When the TR jet is weak
Not every patient gives a clean Doppler signal. In those cases, you can lean on PAAT (acceleration time) a short PAAT (<105ms) suggests high pressures, while a longer time (>130ms) points toward normal pressures. Some clinicians also use the peak velocity of the pulmonary regurgitation jet as a backup.
Reallife anecdote
One of my cardiology fellows, Dr. Lee, remembered a 58yearold woman who came in with fatigue. Her TR jet was barely measurable, but the PAAT was 92ms. That clue prompted a catheterization that revealed severe PH, saving her from years of untreated disease. Its a reminder that a single number rarely tells the whole story.
Benefits and Risks
Why early echo detection matters
Finding PH early gives you a head start on therapy medicines, lifestyle tweaks, and closer monitoring. The sooner you intervene, the better the chance of preserving rightventricular function.
Potential pitfalls of relying solely on echo
Echo is an estimate. Poor acoustic windows, body habitus, or operator inexperience can give false positives (thinking you have PH when you dont) or false negatives (missing a real problem). Thats why most guidelines recommend confirming moderatetosevere echo findings with catheterization.
Balanced decision tree
Heres a quick mental flowchart you can run through after your echo report:
- If PASP<30mmHg likely normal, repeat in 12years if risk factors present.
- If PASP3040mmHg (mild) discuss followup echo in 612months; consider underlying lung disease.
- If PASP>40mmHg (moderatesevere) talk with your cardiologist about rightheart cath.
Clinical Practical Checklist
Before the scan
- Ask the patient to lie flat and breathe normally no deep breaths that could alter IVC size.
- Confirm recent medication list (particularly diuretics) because they can shrink the IVC and lower RAP estimates.
- Gather baseline labs (BNP, troponin) they add context to echo findings.
During the scan
- Obtain TR velocity in multiple windows (apical 4chamber, parasternal) to catch the highest signal.
- Measure IVC diameter 2cm distal to the hepatic vein junction and note collapse on a quick sniff.
- Record PAAT in the right ventricular outflow tract view.
- Take a quick snapshot of RV size and function (TAPSE, FAC) they influence prognosis.
After the scan
- Plug numbers into the PASP formula on a handy worksheet (you can print this page).
- Compare the result with the severity classification table above.
- Flag any moderate or severe values for immediate discussion with the referring physician.
- Schedule a repeat echo if findings were borderline or if symptoms change.
Putting It All Together
Understanding pulmonary hypertension echo criteria isnt about memorizing a jumble of numbers; its about weaving those numbers into a story your heart is telling you. When the echo shows a TR velocity of 3.5m/s and an IVC that barely collapses, the story says my right ventricle is working hard against high pressure and thats a cue to act.
At the same time, you have to respect what echo cant reveal: the exact pressure measured in the pulmonary artery, the response of the lungs, and the underlying cause (whether its leftheart disease, lung disease, or a primary vascular problem). Thats why a balanced approach using echo as a reliable screen, then confirming with catheterization when needed gives you the best chance at a timely, accurate diagnosis.
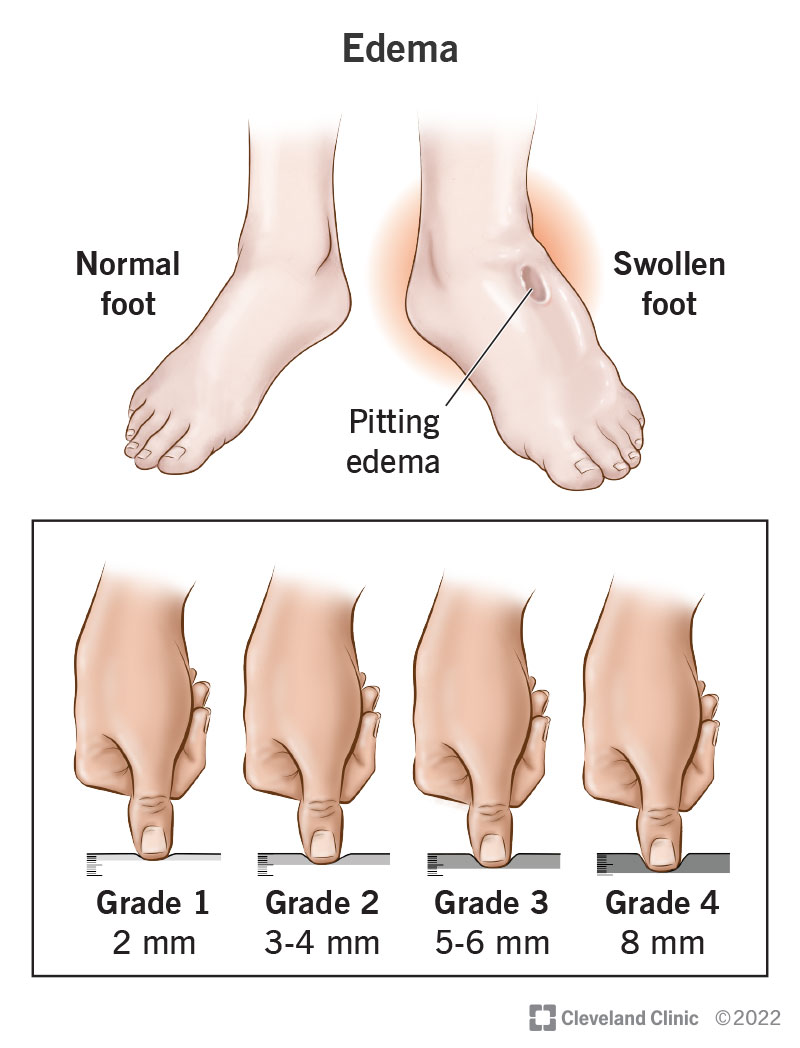
Patients with heart failure often have overlapping signs such as edema or leg swelling that can complicate the picture when present, consider evaluating for heart failure edema as part of your differential diagnosis and management plan.
Conclusion
In a nutshell, the pulmonary hypertension echo criteria give you a fast, noninvasive window into your lungartery pressures. By mastering the key measurements TR velocity, RVSP, PASP, PAAT, and IVCderived RAP you can confidently gauge whether youre looking at mild, moderate, or severe disease. Remember the sweet spot: use echo to flag problems early, but dont let it be the final word when numbers climb into the moderatetosevere range. Pair your echo results with clinical judgment, followup testing, andmost importantlya compassionate conversation with your healthcare team.
Feel empowered? Grab the simple checklist above, bring it to your next appointment, and ask your doctor to walk you through each echo number. Knowledge is the best companion on the road to better heart health.
FAQs
What echocardiographic measurement is primarily used to estimate pulmonary artery pressure?
The peak tricuspid regurgitant velocity (TRV) is used with an estimated right atrial pressure (RAP) to calculate the pulmonary artery systolic pressure (PASP), serving as a surrogate for pulmonary artery pressure.
What are the echo criteria cutoffs for mild, moderate, and severe pulmonary hypertension?
Mild PH: PASP 30-40 mmHg or TRV 2.6-3.0 m/s; Moderate PH: PASP 41-55 mmHg or TRV 3.0-3.4 m/s; Severe PH: PASP >55 mmHg or TRV >3.4 m/s.
How is right atrial pressure (RAP) estimated on echocardiography?
RAP is estimated by assessing the inferior vena cava (IVC) size and its collapsibility during inspiration; a dilated IVC (>2.1 cm) with <50% collapse suggests RAP ~15 mmHg, while a smaller, collapsible IVC suggests RAP ~5 mmHg.
Why is echocardiography used before right heart catheterization in suspected PH patients?
Echocardiography is a quick, noninvasive screening tool that estimates pulmonary pressures and helps identify patients needing confirmatory right heart catheterization, thereby reducing unnecessary invasive procedures.
What other echocardiographic signs support the diagnosis of pulmonary hypertension?
Besides TR velocity and PASP, pulmonary artery acceleration time (PAAT), right ventricular size and function, and pulmonary regurgitation jet velocity are additional parameters that help assess PH probability.