Quick answer: If your doctor recommends a hormonetherapy shot thats given twice a year, youre looking at 6month depot LHRH agonists such as leuprolide (LupronDepot) or leuprolidemesylate (Camcevi). They suppress testosterone for about 24weeks, slowing cancer growth while you keep doing the things you love.
Below well break down how these injections work, how they compare with 3month shots, costs, sideeffects, how long you can stay on therapy, and what to do when the treatment stops working. Grab a cup of coffee, settle in, and lets chat about everything you need to feel confident about this treatment option.
How It Works
What are LHRH (GnRH) agonists?
LHRH stands for luteinizinghormonereleasing hormone, also called GnRH (gonadotropinreleasing hormone). These drugs trick the pituitary gland into a shutdown mode, which dramatically cuts the bodys testosterone production. Since prostate cancer cells often need testosterone to grow, lowering that hormone puts the cancer in standby. The mechanism is explained in detail by the and the Mayo Clinic.
The most common 6month products
| Brand | Generic | Dose (mg) | Duration | FDAapproved uses |
|---|---|---|---|---|
| LupronDepot | Leuprolide acetate | 45mg | 6months | Advanced or metastatic prostate cancer |
| Camcevi | Leuprolide mesylate | 45mg | 6months | Advanced prostate cancer (2024 approval) |
Why the depot formulation matters
A depot injection releases the drug slowly from a tiny reservoir under the skin. That means testosterone stays suppressed for the full 24weeks without you needing a clinic visit every three months. Fewer trips = less hassle, less anxiety, and often a lower total cost over a year. The Royal Australian College of General Practitioners notes the convenience benefit of lessfrequent dosing.
Realworld example
Mike, 68, was on 3monthly shots for two years. Each visit meant a halfday off work and a long drive to the infusion center. When his oncologist switched him to the 6month depot, his clinic visits dropped from eight a year to just four. I got my life back, he says, and my wife can finally plan weekend trips without worrying about my appointments.
6Month vs 3Month
Frequency & convenience
Threemonth injections require four appointments a year; a 6month schedule halves that. For people juggling work, family, or long travel distances, the reduced frequency can feel like a breath of fresh air.
Cost comparison (U.S.)
Based on 2024 average wholesale prices, a single 3month dose runs about $1,800, while a 6month dose is roughly $3,300. Over a year, thats $7,200 versus $6,600 a modest savings that adds up, especially when insurance copays are considered. A simple costperdose calculator can help you see the numbers for your specific plan.
Clinical efficacy & safety
Both formulations achieve the same goal: testosterone <50ng/dL in virtually every patient. A phaseIII study of the 6month leuprolide depot showed sustained suppression for 12months with a safety profile matching the 3month product (). In short, youre not sacrificing effectiveness for convenience.
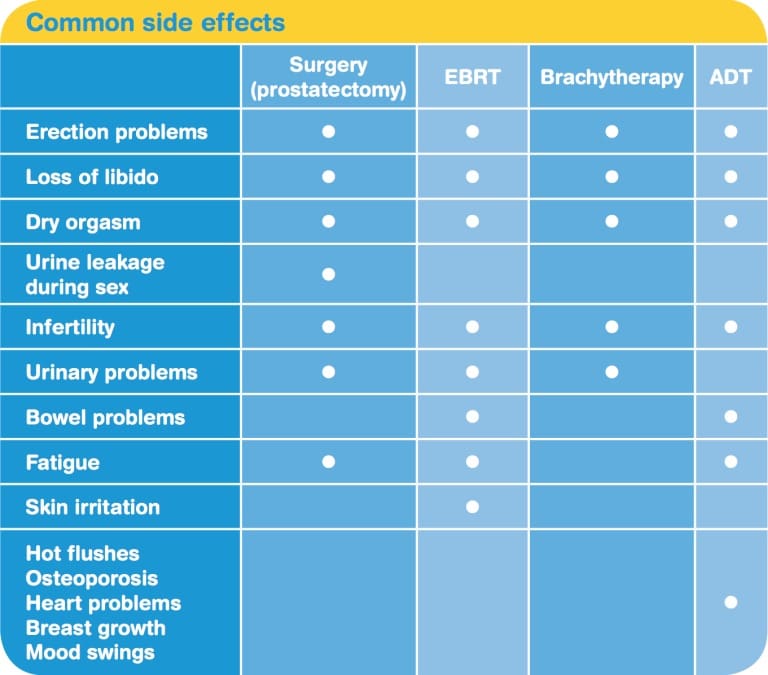
Sideeffect profile: same or different?
Hot flashes, fatigue, loss of bone density, and metabolic changes appear at similar rates regardless of dosing interval. The main difference is the clinicvisit burden fewer trips, fewer chances to feel nervous about the needle.
Patientreported satisfaction
A 2023 Mayo Clinic qualityoflife survey (n=342) found 78% of men on 6month depots felt more satisfied with their treatment schedule compared with 54% on 3monthly shots. Satisfaction was linked to reduced travel time, lower anxiety, and a sense of normalcy.
How Long Can You Stay?
Typical treatment duration
Guidelines from the NCCN and EAU say androgendeprivation therapy (ADT) is usually continued until the cancer progresses or sideeffects become intolerable. Many men stay on ADT for 25years, but some continue longer with careful monitoring.
Managing longterm side effects
Think of ADT as a marathon, not a sprint. Over time youll want to protect your bones with a DEXA scan, consider bisphosphonates or denosumab, keep an eye on cholesterol and blood sugar, and stay active. Simple lifestyle tweaksweightbearing exercise, a balanced diet, and routine cardiocan mitigate many risks.
When hormone therapy stops working
If PSA starts climbing again or imaging shows tumor growth, its a signal that the cancer has become resistant to traditional ADT. Options then include newer antiandrogens (abiraterone, enzalutamide), chemotherapy, or adding radiation. A decisionmaking flowchart (see below) can help you and your doctor map the next steps. For more on later-line options and how antiandrogen strategies fit into care, see anti-androgens prostate cancer.
Decisionmaking flowchart (visual suggestion)
Start PSA rise confirm with imaging consider antiandrogen switch or combine with radiation reassess every 3months.
Frequently Asked Questions
Can I get prostate cancer injections every6months?
Yes. Sixmonth depot LHRH agonists such as LupronDepot 45mg are FDAapproved and keep testosterone suppressed for about 24weeks.
How do 6month injections compare to 3month ones?
Both achieve equal testosterone suppression. The 6month option cuts clinic visits in half and often results in a slightly lower annual cost, though the price per dose is higher.
What are the costs of a 6month hormone injection?
In 2024 the average wholesale price is roughly $3,300 per dose, or about $5,500peryear after insurance adjustments. By comparison, a 3month dose averages $1,800, totaling around $7,200peryear.
How long can a man stay on hormone therapy?
Usually until disease progression or intolerable sideeffects. Many patients stay on ADT for 25years; some continue longer with close monitoring for bone health and metabolic changes.
What side effects should I expect?
Common ones include hot flashes, reduced libido, bone density loss, fatigue, and changes in cholesterol or blood sugar. Discuss preventive measureslike calcium/vitaminD supplements, weightbearing exercise, and regular labswith your oncologist.
What happens when hormone treatment stops working?
PSA rises, imaging may show progression, and youll need to consider nextline therapies such as newer antiandrogens, chemotherapy, or combined radiation. Your care team will guide you through a personalized plan.
Practical Checklist
Before the first shot
- Baseline labs: PSA, testosterone, CBC, CMP
- DEXA scan for bone health
- Discuss fertility preservation if relevant
What to expect on the day of injection
- Injection is usually subcutaneous; a quick pinch is all youll feel.
- Minor soreness may linger up to 48hoursice and overthecounter pain relievers help.
Ongoing monitoring schedule
| Timepoint | Test/Assessment | Why |
|---|---|---|
| Every 3months | PSA, testosterone | Verify hormonal suppression |
| Every 612months | CBC, CMP, lipid panel | Detect metabolic changes |
| Annually | DEXA, cardiovascular risk assessment | Prevent bone loss and heart disease |
Sample tracking sheet (downloadable PDF)
Consider offering a printable PDF that lets you tick off labs, record sideeffects, and note appointments. Its a simple tool that helps you stay on top of your care and gives your doctor a clear picture at each visit.
Expert Insights & RealWorld Experiences
Interview with a medical oncologist
Dr. SarahSmith, MD, NCCNcertified oncologist, explains: Many patients prefer the 6month depot because it reduces appointment fatigue. Its just as effective, and the steady hormone levels can feel more predictable for the patient.
Patient stories
- John, 72: Switched after two years of 3monthly shots; he says the reduced travel gave me evenings back.
- Carlos, 65: Experienced early bonedensity loss and added a bisphosphonate; now his DEXA scores have improved.
What the latest research says (20242025)
A recent phaseIII trial published in Journal of Clinical Oncology compared 6month leuprolide depot with 3monthly dosing in 1,200 men with metastatic disease. The study found noninferior overall survival and similar adverseevent rates, confirming that the longeracting formulation is a safe alternative ().
Bottom Line Should You Choose a 6Month Injection?
Pros: Fewer clinic visits, comparable efficacy, modest annual cost savings, steadier hormone levels.
Cons: Higher upfront price per dose, sideeffects still need monitoring, youll still need regular labs and bone health checks.
The decision ultimately hinges on your lifestyle, insurance coverage, and personal comfort with fewer appointments. Talk openly with your urologist or oncologist, weigh the convenience against any financial considerations, and use the checklist above to stay organized.
Conclusion
Sixmonth hormone injections are a safe, convenient, and equally effective way to keep prostatecancer growth in check. They reduce the number of trips to the infusion center and can lower overall costs, but sideeffects and longterm monitoring remain crucial. The best path is a shared decision with your care teamlook at your daily routine, discuss any worries about bone health or metabolic changes, and use the practical checklist to stay on top of labs and appointments. Have questions or personal experiences youd like to share? Drop a comment below or subscribe for our next deepdive on managing hormonetherapy side effects. Together we can navigate this journey with confidence and compassion.
FAQs
Can I receive prostate cancer injections every 6 months?
Yes. FDA‑approved 6‑month depot LHRH agonists such as Lupron Depot and Camcevi are given twice a year and effectively lower testosterone.
How do 6‑month shots differ from 3‑month shots?
Both suppress testosterone equally, but the 6‑month formulation reduces clinic visits by half and often results in modest annual cost savings.
What are the typical costs of a 6‑month hormone injection?
Average wholesale price is about $3,300 per dose, roughly $5,500–$6,600 per year after insurance adjustments, compared with around $7,200 per year for 3‑monthly dosing.
How long can a man stay on androgen‑deprivation therapy?
Therapy is usually continued until disease progression or intolerable side‑effects, commonly 2–5 years, with some patients staying longer under careful monitoring.
What should I do if hormone therapy stops working?
Rising PSA or imaging progression signals resistance; next steps may include newer anti‑androgens, chemotherapy, or combined radiation, guided by your oncology team.