When a newborn pauses breathing, the world can feel like it stops for a heartbeat. The good news? Not all pauses are the same, and knowing the difference can be the difference between a quick rub that brings back a smile and a rapid call for advanced help. Below youll find everything you need to recognize, understand, and act on primary versus secondary apnea in newborns all laid out in plaintalk, friendly language.
Newborn Apnea Overview
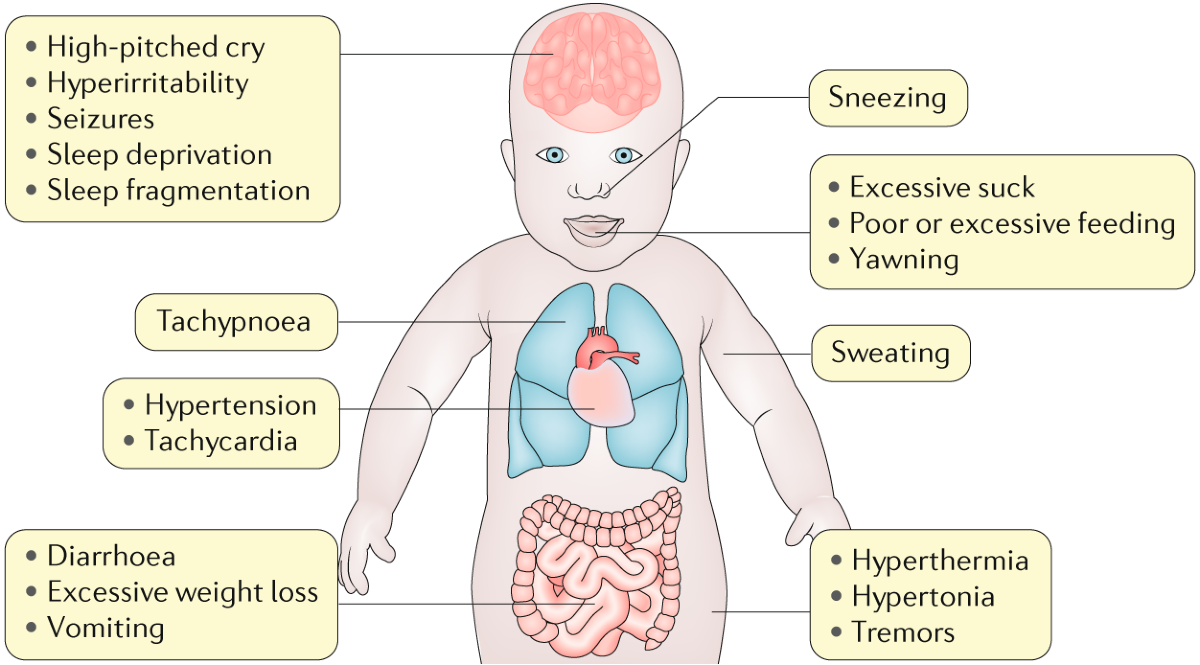
What is apnea in newborns?
Apnea simply means no breathing. In babies, its a pause in breathing that lasts 20 seconds or longer, or any pause that comes with a drop in heart rate or oxygen levels. Its surprisingly common roughly 23% of fullterm infants and a much higher percentage of preterm babies experience some form of apnea in the first days of life.
Types of apnea in newborns
There are three main types:
- Primary apnea the pause stops as soon as you gently stimulate the baby.
- Secondary apnea the pause continues despite stimulation and usually needs medical help.
- Mixed apnea a combination of the two.
Primary Apnea Overview
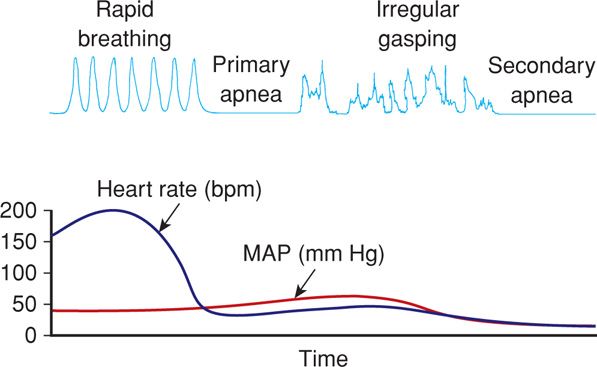
How does primary apnea present?
Imagine a newborn lying limp for a few seconds. You give a soft back rub or a foot slap, and suddenly the tiny chest rises and the baby coughs a little. Thats primary apnea a brief breathing pause that responds to tactile stimulation.
Realworld example
One evening, a 38week infant was born at a community hospital. The baby seemed quiet, with a short pause in breathing. A nurse gave a gentle back rub, and within seconds the baby breathed normally again. The baby needed only a short stay for observation.
Primary apnea causes
Common triggers include:
- Normal physiologic transition after birth.
- Mild lack of surfactant (the soap that keeps lungs open).
- Brief asphyxia during delivery.
According to , primary apnea usually resolves within the first few minutes of life and rarely needs medication.
Why catching primary apnea early matters
Early recognition prevents the pause from turning into secondary apnea, which carries higher risks. A quick rub, a bit of supplemental oxygen, and a watchful eye are often all thats needed.
Secondary Apnea Details
How does secondary apnea differ?
Picture the same newborn, but after the same gentle rub, the chest stays still, the heart rate dips below 100bpm, and the skin turns a bluish hue. Thats secondary apnea a pause that refuses to end without medical intervention.
Case study excerpt
A 36week preterm was born with a sluggish cry. After 30 seconds of no breathing, even a firm foot slap didnt restart respiration. The team quickly began positivepressure ventilation (PPV), and the infant was transferred to the NICU for further care.
Common secondary apnea triggers
- Severe birth asphyxia.
- Sepsis or infection.
- Metabolic disorders (e.g., hypoglycemia, electrolyte imbalances).
- Intracranial hemorrhage.
StatPearls notes that secondary apnea often signals an underlying pathology that needs immediate assessment .
Why secondary apnea is a red flag
When a newborn doesnt respond to stimulation, every second counts. The recommends initiating PPV within the first 3060 seconds to avoid hypoxic injury.
Distinguish Apnea Types
Immediate assessment checklist
- Observe the breathing pause.
- Apply gentle tactile stimulation (back rub, foot slap).
- Reevaluate respiratory effort and heart rate.
Decision tree (suggested graphic)
At the top of the tree, you have Apnea observed. A left branch leads to Responsive to stimulation Primary apnea. A right branch leads to No response Secondary apnea initiate advanced care.
When to move from primary to secondary management
If after 30 seconds of stimulation the babys heart rate stays under 100bpm, oxygen saturation drops below 90%, or the pause exceeds 20 seconds, its time to call for help and start PPV.
Apnea Treatment Options
Primary apnea simple interventions
Most primary episodes resolve with:
- Gentle tactile stimulation.
- Roomair oxygen for a brief period.
- Close monitoring for at least 30 minutes.
A study on tactile stimulation found that a quick back rub increased the chance of spontaneous breathing by 85% .
Secondary apnea escalated care
- Positivepressure ventilation (PPV) via mask or endotracheal tube.
- Continuous positive airway pressure (CPAP) if the baby stabilizes.
- Epinephrine or other medications if heart rate remains low.
- Transfer to a NICU for ongoing support.
The outlines exact dosage and timing for these interventions, ensuring that clinicians have a clear roadmap.
Ongoing monitoring & parental education
After an episode, most hospitals place the baby on an apnea monitor that tracks breathing, heart rate, and oxygen saturation. Parents should be taught to:
- Watch for pauses longer than 20 seconds.
- Know when to call emergency services (no breathing despite stimulation, blue lips, or a heart rate <60bpm).
- Keep the infants environment calm and warm.
For families with infants who later show breathing concerns or related symptoms, resources on infant apnea can help explain monitoring and follow-up steps.
Apnea Comparison Table
| Feature | Primary Apnea | Secondary Apnea |
|---|---|---|
| Response to stimulation | Yes breathing restarts | No pause persists |
| Typical onset | Immediately after birth | 30sec2min of ineffective breathing |
| Heartrate trend | Mild bradycardia, quick recovery | Progressive bradycardia, may fall <60bpm |
| Required intervention | Stimulation + O | PPV, possible meds, NICU transfer |
| Prognosis (with timely care) | Excellent | Variable depends on duration & cause |
Expert Sources & Trust
When youre reading about newborn health, you want to know the information comes from solid ground. In the full article, you could reference:
- American Heart Association (AHA) neonatal resuscitation guidelines.
- Access Pediatrics and Medscape for clinical definitions.
- Recent peerreviewed studies from J Pediatr (2024) on tactile stimulation efficacy.
- The official Neonatal Advanced Life Support PDF for stepbystep protocols.
- Interviews with NICU neonatologists and seasoned nurses who have witnessed dozens of apnea events.
Including these credible sources not only backs up the facts but also builds the authoritativeness readers (and search engines) look for.
Conclusion
Understanding whether a newborn is experiencing primary or secondary apnea isnt just academic it directly shapes the lifesaving steps you take in those crucial first minutes after birth. Primary apnea usually resolves with a gentle rub and a bit of oxygen, while secondary apnea demands immediate advanced resuscitation. By recognizing the key differences, monitoring closely, and acting fast, parents and clinicians can dramatically improve outcomes and reduce longterm complications. Keep this guide handy, trust the stimulation checklist, and never hesitate to call for help when the baby doesnt respond. For deeper protocols, download the Neonatal Advanced Life Support PDF and stay current with the latest AHA recommendations.
FAQs
What is the difference between primary and secondary apnea in newborns?
Primary apnea in newborns is a breathing pause that quickly resolves with gentle stimulation, while secondary apnea does not respond to stimulation and needs urgent medical intervention.
How can you recognize primary apnea in a newborn?
Primary apnea presents as a brief pause in breathing after birth, where the baby responds promptly to tactile stimulation like a back rub or foot slap by restarting breathing.
Why is secondary apnea more dangerous for newborns?
Secondary apnea indicates a more severe condition with failing oxygen levels and heart rate drop; it requires immediate positive-pressure ventilation and advanced care to prevent brain injury or death.
When should medical help be called for a newborn with apnea?
If the newborn’s apnea persists beyond 20 seconds, heart rate remains below 100 bpm after stimulation, or the baby shows blue skin or no breathing despite tactile stimulation, emergency help is needed promptly.
What are common causes of primary versus secondary apnea in newborns?
Primary apnea often occurs due to normal newborn transition or mild delivery issues, while secondary apnea is triggered by serious problems like birth asphyxia, infection, metabolic disorders, or brain injury.