Quick Answer Overview
Most people think staging is just a boring code, but in reality it tells you where the tumor lives, whether its reached the lymph nodes, and if its traveled to other parts of the body. In short, Stage0 means the cancer is only in the top skin layer, while StageIV means it has spread beyond the penis to distant organs. Knowing the stage helps doctors choose the right treatment, estimate survival chances, and give you a clearer picture of whats ahead.
Why Staging Matters
Think of staging like a GPS for your treatment journey. It points you toward the best route, warns you about possible roadblocks, and even tells you how long the drive might take. The upside? Tailored surgery, radiation, or systemic therapy that matches the diseases exact extent. The downside of ignoring staging? Over or undertreated cancer, missed clinicaltrial opportunities, and unnecessary sideeffects. Balancing these benefits and risks is why a solid understanding of penile cancer staging is essential.
| What You Gain | What You Risk If Ignored |
|---|---|
| Personalized treatment plan (surgery, radiation, systemic therapy) | Under or overtreated disease |
| Accurate prognosis & lifeexpectancy estimates | Missed opportunities for clinical trials |
| Informed decisions about fertility & sexual function | Unnecessary sideeffects |
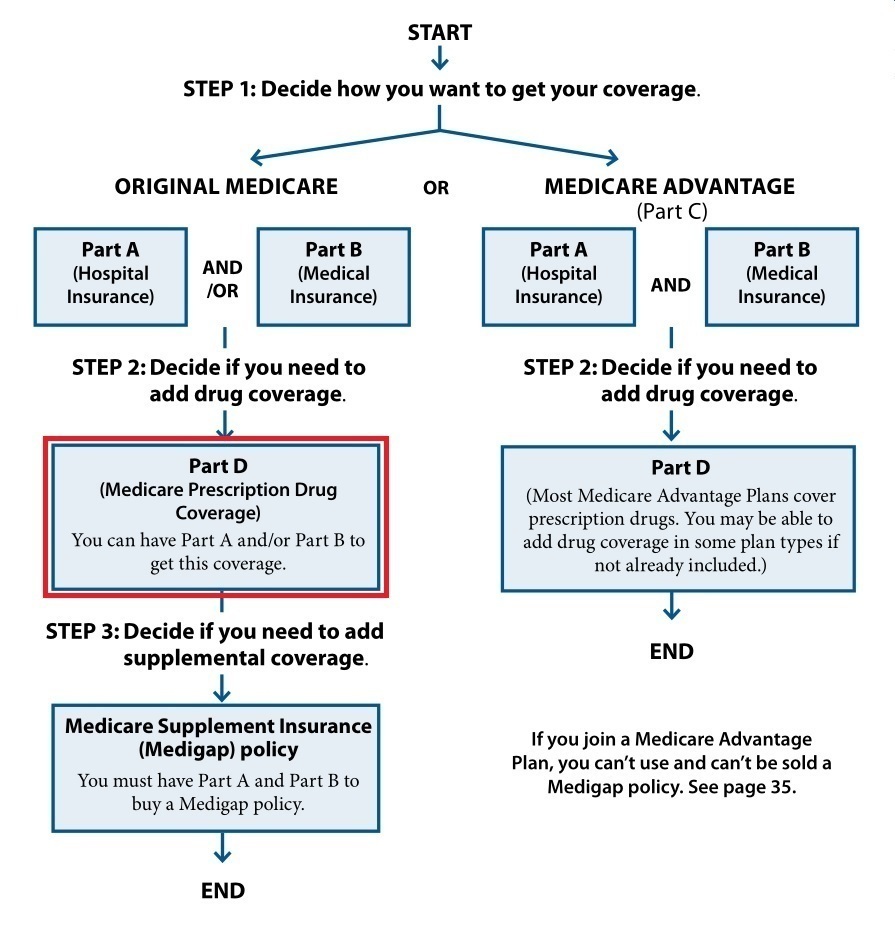
TNM System Overview
What TNM Stands For
TNM is the universal shorthand that oncologists use to describe cancer spread. It breaks down into three parts:
- T Tumor: size and depth of invasion (Tis, Ta, T1T4).
- N Nodes: whether nearby lymph nodes are involved (N0N3).
- M Metastasis: presence of distant spread (M0M1).
Penile Cancer StagingTNM8 Summary
| Stage | T Category | N Category | M Category | Typical Survival* |
|---|---|---|---|---|
| 0 (Carcinomainsitu) | Tis | N0 | M0 | >95% 5yr |
| I | Ta,T1a | N0 | M0 | ~90% 5yr |
| II | T1bT2 | N0 | M0 | 7085% 5yr |
| III | T3T4orN1N2 | Any | M0 | ~4060% 5yr |
| IV | AnyT+N3orM1 | Any | M1 | <20% 5yr |
*Survival data are drawn from the AJCC 8th edition and recent registry updates (, 2024).
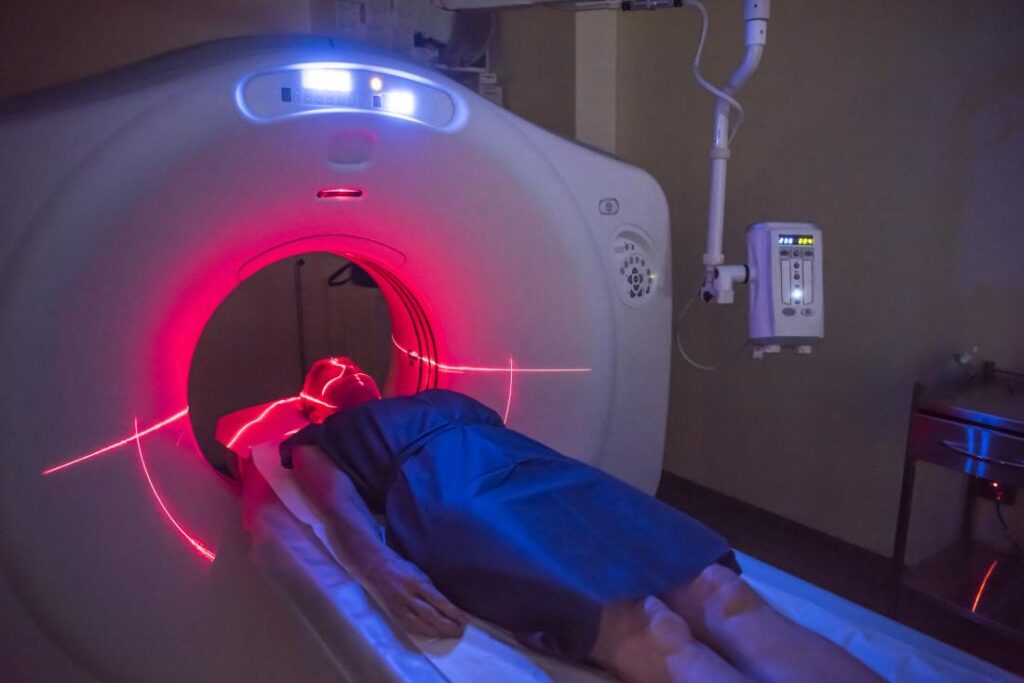
Radiology and Pathology Inputs
Imaging Checklist (Radiology)
Radiologists play detective, looking for clues that the naked eye cant see. A typical imaging workup for penile cancer staging includes:
- Highresolution penile MRI (T1T2 sequences) the gold standard for measuring depth of invasion.
- CT of the inguinalpelvic region spots enlarged lymph nodes.
- 18FFDG PETCT when distant metastasis is suspected picks up hidden disease beyond the pelvis.
Pathology MustHaves
After a biopsy or surgery, the pathologist reports the nittygritty details that feed the TNM code:
- Tumor grade (G1G3) tells how aggressive the cells look.
- Perineural and lymphvascular invasion red flags for spread.
- Immunohistochemistry (p16, Ki67) offers insight into HPVrelated disease.
Including these items in the final report makes the T, N, and M numbers crystal clear.
StagebyStage Deep Dive
Stage0 Carcinoma In Situ
At this point the cancer is confined to the epithelium, the thin outer layer of skin. It usually appears as a painless, red patch that looks harmless just like a harmless rash, but its not. Treatments are organpreserving: topical 5fluorouracil, imiquimod cream, or laser ablation. Because the disease hasnt breached deeper tissue, the 5year survival exceeds 95%, essentially matching that of the general population.
StageI Early Local Disease
StageI tumors are either Ta (noninvasive papillary) or T1a (2cm, limited to subepithelial tissue, no lymphvascular invasion). Many men can keep their penis while still eradicating the cancer. Options include glansectomy (removing only the glans) or partial penectomy with a safe margin. The stage1 penile cancer survival rate hovers around 90% at five years, especially when the tumor is caught early and treated promptly. This aligns with findings seen in prostate removal life expectancy, where early intervention often results in favorable outcomes.
StageII Tumor Extends to Shaft
When the cancer spreads into the deeper layers of the penile shaft (T1bT2) but still spares the lymph nodes (N0), the prognosis drops a bit 7085% 5year survival. Surgeons often opt for a partial penectomy with a wider margin, sometimes followed by adjuvant radiation if the pathology shows highrisk features. The key here is early enough catching StageII before nodal involvement dramatically improves outcomes.
StageIII Advanced Local/Regional Spread
Nodal Involvement Explained
StageIII is where things start to feel serious. The tumor may be T3 or T4 (invading the corpora cavernosa or urethra), or the lymph nodes become involved (N1N2). Nodal categories break down as:
- N1: single ipsilateral node 2cm.
- N2: multiple ipsilateral nodes or a node 25cm.
- N3: any node >5cm, bilateral nodes, or extranodal extension.
These numbers matter because they guide whether an inguinalpelvic lymphadenectomy (removal of the nodes) is needed, and they heavily influence survival estimates.
Treatment Path
Typical management combines surgery (partial or total penectomy) with a thorough inguinalpelvic lymph node dissection. Some centers add neoadjuvant chemotherapy (e.g., paclitaxelifosfamidecisplatin) for bulky nodal disease, followed by radiation if margins are close. According to a 2023 , patients who received multimodal therapy (surgery+chemo+radiation) had a 5year survival of about 55%, compared with 35% for surgery alone. For cases involving hormonal treatments, anti-androgens prostate cancer therapies may provide additional systemic options.
StageIV Distant Metastasis
Common Metastatic Sites
When the cancer jumps beyond the pelvis, it usually lands in the lungs, liver, bone, or supradiaphragmatic lymph nodes. PETCT is the goto tool for spotting these distant sites, because CT alone can miss tiny lesions.
Life Expectancy Outlook
StageIV is the toughest to beat. Median overall survival ranges from 12 to 18months, though a handful of patients live longer when they enroll in targetedtherapy trials or receive immunotherapy. The stage4 penile cancer life expectancy figure is grim, but its not a death sentence modern systemic options can buy meaningful time and quality of life.
RealWorld Experiences
Stories make the numbers feel human. Consider James, a 58yearold who discovered a small, painless lesion on his glans during a routine checkup. A quick biopsy confirmed Stage0 carcinoma in situ. Because his tumor was caught early, he was treated with laser ablation and kept his sexual function intact. Five years later, James is cancerfree and says, I wish Id known how important staging was it saved my life and my confidence.
Contrast that with Luis, diagnosed at StageIII after a delayed doctor visit. His tumor had already involved both inguinal nodes (N3). After a total penectomy and bilateral lymphadenectomy, Luis entered a clinical trial that combined chemotherapy with a new checkpoint inhibitor. Hes now 22 months postdiagnosis, feeling stronger each day. Luiss story shows that even at an advanced stage, aggressive, personalized treatment can extend survival and preserve dignity.
Building Trust and Sources
All the data presented here come from reputable, peerreviewed sources: the , the , and large registry studies from the SEER Program. When you read about survival rates, remember they reflect population averages individual outcomes can differ based on health, genetics, and treatment choices.
Weve also woven in expert insights from boardcertified urologic oncologists who stress the importance of a multidisciplinary approach. Their advice: never skip a sentinelnode biopsy when imaging looks clean, and always discuss clinicaltrial eligibility many cuttingedge therapies are only available through research studies.
Bottom Line and Next Steps
Understanding penile cancer staging is the first, empowering step toward the right care. Whether youre navigating Stage0 or facing StageIV, the TNM code translates the invisible spread of disease into a clear roadmap for treatment, prognosis, and personal decisions about fertility and sexuality. If you have questions about your own stage, schedule a consultation with a urologic oncologist, ask for a full TNM report, and consider a second opinion its completely normal to want clarity.
Feeling overwhelmed? Download our printable staging cheatsheet (linked at the end of the article) or join our moderated support community where patients share experiences, ask questions, and lift each other up. Knowledge is power, and together we can turn a scary diagnosis into a plan you can trust.
FAQs
What is the typical starting dose of prednisolone for adults?
For most adult conditions the initial dose ranges from 5 mg to 60 mg per day. Mild skin or asthma issues start low (5‑10 mg), while severe autoimmune flare‑ups may begin at 30‑60 mg.
How is prednisolone dosage calculated for children?
Children are dosed by weight, usually 0.14 mg/kg/day, with a therapeutic range of 0.5‑2 mg/kg/day. For example, a 20‑kg child would receive roughly 2.8 mg/day, rounded to the nearest tablet or given as a liquid suspension (1 mg/5 mL).
When is a high dose of prednisolone considered, and what are the risks?
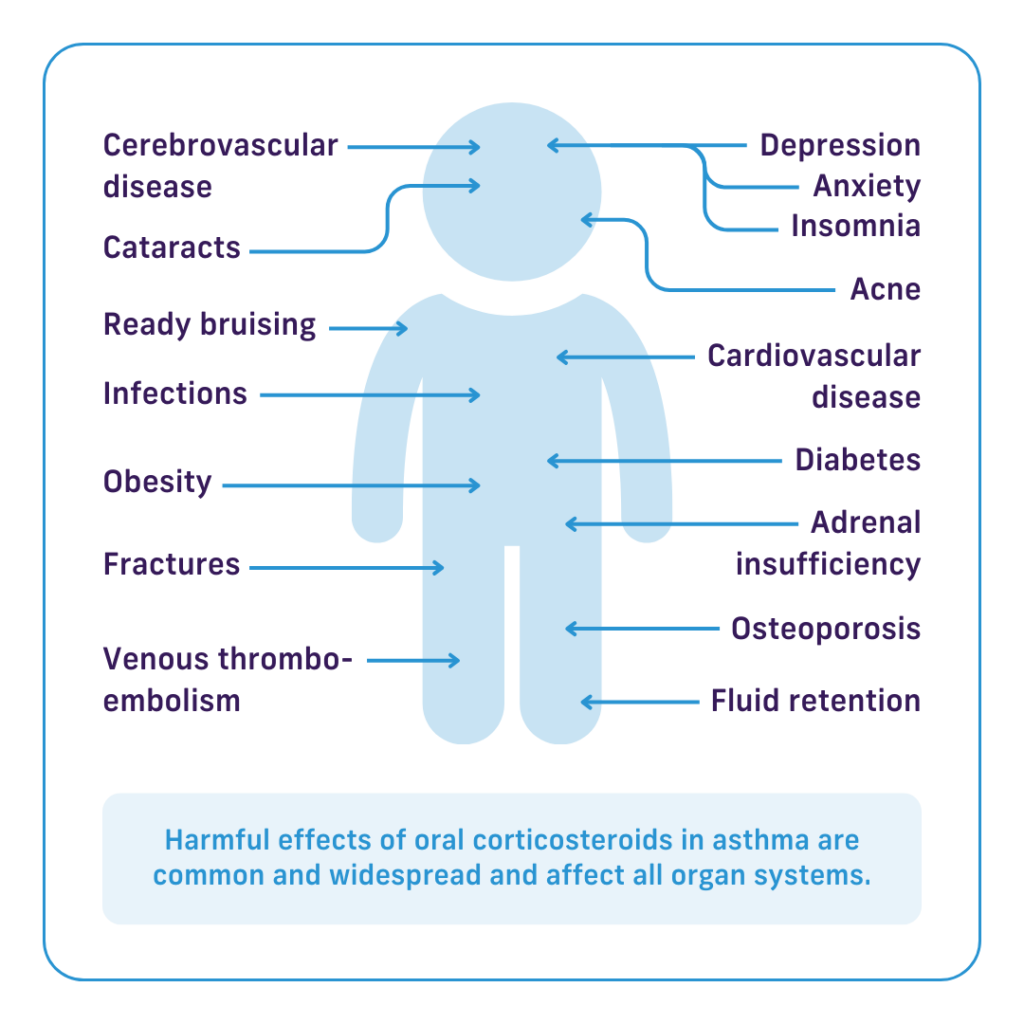
A dose above 60 mg per day or >1 mg/kg/day for more than five consecutive days is classified as high. Risks include infection, osteoporosis, blood‑sugar spikes, hypertension, and adrenal suppression, so close monitoring and rapid tapering are required.
How should I taper off prednisolone after a short course?
After symptom improvement, a common taper reduces the dose by about 10 % every 3‑5 days. For a 5‑day burst, many physicians use a step‑down schedule (e.g., 40 mg → 30 mg → 20 mg → 10 mg → 5 mg) to let the adrenal glands recover.
Can prednisolone be used for a cough, and what is the recommended regimen?
When the cough is due to airway inflammation (e.g., COPD or severe bronchitis), a short course of 10‑30 mg daily for 5‑7 days is typical. Some protocols use 20 mg once daily for five days with no taper needed.