Are you wondering whether surgery could finally calm the pressure spikes that keep you up at night? The short answer is: yes, there are several proven surgical routes that can protect your vision, but each comes with its own set of pros and cons. Below we'll walk through why surgery sometimes becomes necessary, what the main procedures are, and how you can decide which path feels right for you.
When Surgery Becomes Needed
Most of us start with eye drops or laser tricks, hoping the pressure (IOP) will stay under control. When it doesn't, a surgeon steps in. Common triggers include:
- IOP stubbornly >21mmHg despite maxtolerated medication.
- Progressive loss in visualfield tests that shows up even though you're diligent about drops.
- Sideeffects from medications that make daily life uncomfortable.
According to a recent survey of glaucoma specialists, roughly 1520% of pigmentary glaucoma patients eventually require surgery, especially those with a younger age profile and a myopic eye.
How Common Is Surgery in Pigmentary Glaucoma?
While pigmentary glaucoma itself accounts for just 0.41% of all glaucoma cases, the need for surgical intervention is far less commonstill, for those who do need it, the outcomes can be lifechanging. If cataract or lens changes are the underlying trigger for pigment release, addressing the lens may be part of the solution; sometimes a targeted approach such as cataract surgery glasses discussions becomes relevant when planning combined care.
Overview of Options
| Procedure | Setting | Typical Candidates | Key Advantage | Major Risk |
|---|---|---|---|---|
| Argon Laser Trabeculoplasty (ALT) | Officelaser | Earlymoderate PG uncontrolled on meds | Minimal downtime | IOP rebound over time |
| Laser Peripheral Iridotomy (LPI) | Officelaser | Pigment dispersion with angleclosure component | Prevents pupillary block | Rare dysphotopsia |
| Trabeculectomy | Operating room | Advanced or refractory PG | Proven longterm IOP control | Hypotony, bleb infection |
| Glaucoma Drainage Implant | Operating room | Failed trabeculectomy or highrisk eye | Consistent IOP reduction | Platerelated complications |
| Canaloplasty (Microinvasive) | Operating room | Patients preferring blebfree surgery | Preserves conjunctiva | Limited longterm data |
| IOL Exchange (Lensrelated) | Operating room | Lensinduced pigment release | Removes pigment source | Surgical complexity |
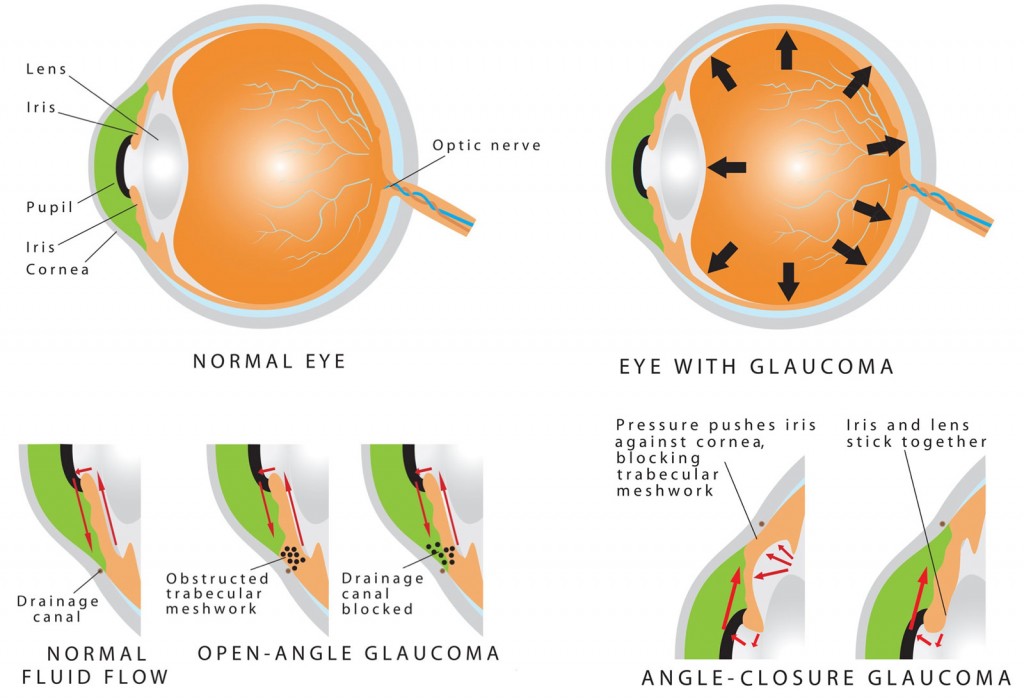
Choosing Laser vs. Incisional Surgery
Laser procedures like ALT and LPI are often the first line because they're quick, painless, and don't need a cut. However, if the eye keeps leaking pigment into the trabecular meshwork, an incisional surgerytrabeculectomy, a drainage device, or canaloplastyoffers deeper, more durable pressure control.
StepbyStep Procedures
Argon Laser Trabeculoplasty (ALT)
Preprocedure Checklist
We'll verify baseline IOP, run a gonioscopy to see the angle, and rule out active inflammation. If you're on a prostaglandin drop, we usually pause it 24 hours before the laser.
How the Laser Works
Using a tiny spot of orangered light, the surgeon delivers 50100 burns to the trabecular meshwork. The heat causes the tissue to shrink slightly, creating tiny tunnels that let fluid flow out more easily.
Aftercare
Topical steroids for a week, a followup IOP check at Day 1, Week 1, and then Month 1. Most patients see a 2030% pressure drop that holds for 12 years before the effect tapers.
Trabeculectomy
Surgical Technique in a Nutshell
Think of it as building a tiny drainage tunnel under the eye's surface. A thin flap is made in the sclera, a small window (the ostomy) is created, and antimetabolites like mitomycinC are applied to keep the site from scarring shut.
Recovery Milestones
- Day 1: Check for a shallow, wellformed bleb.
- Week 1: Most patients can resume light activities.
- Month 1: IOP should settle; we adjust drops if needed.
Common Complications in Pigmentary Glaucoma
Because pigment can occasionally clog the new drainage pathway, there's a slightly higher risk of bleb failure. Prompt postoperative monitoring helps catch problems early.
Glaucoma Drainage Implant
Implant surgery places a tiny silicone or polypropylene plate behind the eye, attached to a tube that shunts fluid to a reservoir. It's a solid choice when previous trabeculectomy has failed.
Canaloplasty (Microinvasive)
Canaloplasty threads a microcatheter 360 around Schlemm's canal, inflating a tiny balloon to open the drainage channels without creating a bleb. Early studies show an average IOP reduction of 3540% with fewer surface complications.
Risks, Benefits & Prognosis
Every surgical road has its traffic signs. Let's break them down.
Balancing Upsides and Downsides
Benefits: Most procedures lower IOP by 3050%, slowing or halting visualfield loss. In many cases, patients can drop or even stop their eyedrop regimen, which feels like a weight lifted off daily life.
Risks: Bleeding, infection, hypotony (too low pressure), and for some, a need for additional surgery down the line. Rarely, pigmentary glaucoma can lead to blindness if pressure stays uncontrolled; surgery dramatically reduces that risk.
LongTerm Outlook
Data from major ophthalmology bodies suggest that after a successful trabeculectomy, more than 80% of patients maintain stable visual fields for at least 5 years. Canaloplasty shows promising 3year results, but we still need longer studies to confirm durability.
Does Pigmentary Glaucoma Cause Blindness?
It can, but only when the pressure never settles. Think of the eye's drainage system as a highway: if traffic (aqueous humor) keeps piling up, the bridge (optic nerve) gets damaged. Surgery clears the jam, preserving the view.
Preparing for Surgery
PreOperative Workup
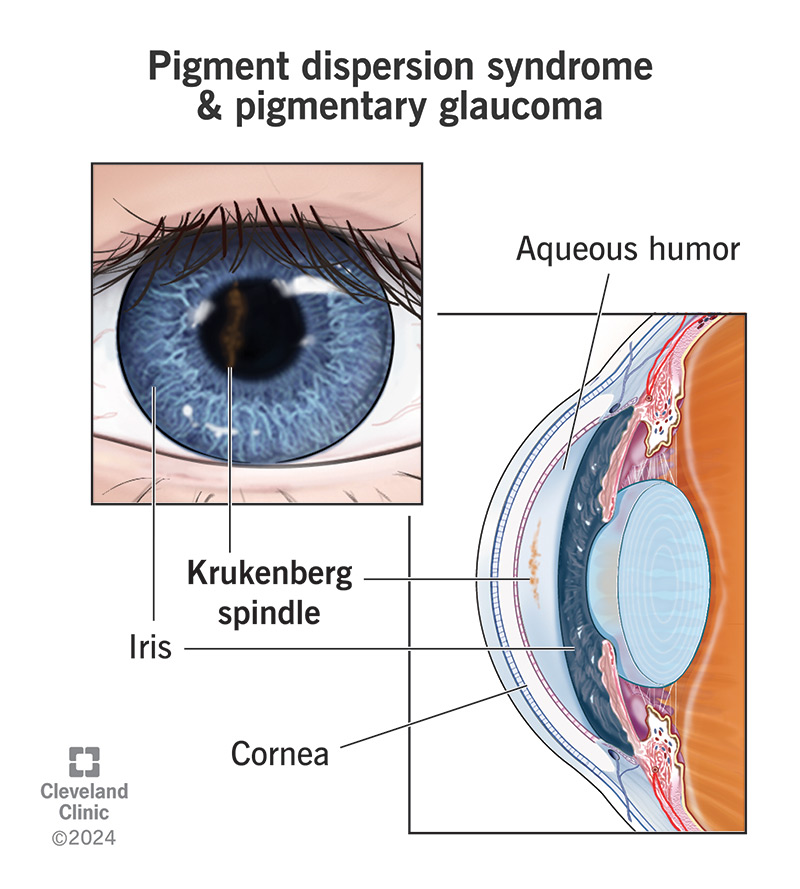
We'll order a full visualfield test, OCT imaging of the optic nerve, and a detailed gonioscopy to map pigment deposition. If you've ever heard of the Krukenberg spindle, that's one of the signs we look for on the cornea.
Medication Adjustments
Prostaglandin analogues can cause a pigment flare after laser, so we often pause them a few days before surgery. Anticoagulants? Your cardiologist and our team will coordinate a safe plan.
Choosing a Surgeon
- Boardcertified glaucoma fellowship.
- High volume of pigmentary glaucoma cases (experience matters!).
- Patient testimonials that resonate with you.
Setting Realistic Expectations
Most patients see a pressure drop within the first week, but the final IOP may settle over 46 weeks. Vision won't improve dramaticallysurgery preserves what you have, not restores lost sight.
PostOp Care & LongTerm FollowUp
Immediate Regimen
We prescribe a mild steroid (e.g., prednisolone acetate) 45 times a day for the first week, then taper. Antibiotic drops protect against infection for about a week.
IOP Monitoring Schedule
- Day 1: Quick check for leaks or high pressure.
- Week 1: Evaluate bleb appearance or tube function.
- Month 1, 3, 6, then every 612 months: Full exam and visualfield test.
RedFlag Signs
If you feel sudden pain, notice a rapid drop in vision, or see a watery bubble on the eye surface, call us right awaythese could signal a leak or infection.
When Additional Intervention Is Needed
Some eyes require a needling procedure to revive a failing bleb, or a revision surgery if the tube becomes obstructed. The good news? Most revisions are quick and have excellent outcomes.
Choosing the Right Procedure
| Goal | Best Match | Why |
|---|---|---|
| Minimal downtime | ALT or LPI | Officebased, no incision. |
| Maximum IOP lowering | Trabeculectomy | Proven track record for deep pressure reduction. |
| Blebfree preference | Canaloplasty | Preserves conjunctiva, fewer surface complications. |
| Failed previous surgery | Drainage Implant | Offers reliable drainage when bleb won't work. |
Think of this table as a quickreference menupick the dish that satisfies both your appetite for safety and your craving for effectiveness.
Conclusion
In a nutshell, pigmentary glaucoma surgery can be the turning point that steadies your eye pressure, shields your optic nerve, and lets you ditch the endless cycle of drops. The decision isn't onesizefitsall; it hinges on how aggressive the disease is, your lifestyle, and how comfortable you feel with each option's risk profile. Talk openly with a seasoned glaucoma specialist, ask lots of questions, and remember that you're not alonemany have walked this road and emerged with clearer, more stable vision.
If you've read this far, congratulations! You've taken the first step toward informed empowerment. Got a story about your own surgery journey or a question that's still nagging at you? Drop a comment below or share your experiencetogether we'll keep the conversation going and help each other see a brighter future.
FAQs
What are the common surgical options for pigmentary glaucoma?
Surgical options include Argon Laser Trabeculoplasty (ALT), Laser Peripheral Iridotomy (LPI), trabeculectomy, glaucoma drainage implants, canaloplasty, and intraocular lens exchange for lens-related pigment release.
When is surgery typically recommended for pigmentary glaucoma?
Surgery is recommended when intraocular pressure remains above 21 mm Hg despite medications, progressive visual field loss occurs, or side effects from medications are intolerable.
What are the major risks associated with pigmentary glaucoma surgery?
Risks vary by procedure and can include temporary pressure spikes, bleb infection or failure, hypotony (low eye pressure), bleeding, and plate-related complications with implants.
How effective is trabeculectomy for pigmentary glaucoma?
Trabeculectomy offers proven long-term intraocular pressure control, with over 80% of patients maintaining stable visual fields for at least five years after successful surgery.
Can pigmentary glaucoma surgery restore lost vision?
No, surgery primarily prevents further vision loss by controlling intraocular pressure; it does not restore vision already lost due to optic nerve damage.