Ever wonder why a tiny speck of pigment in the back of your eye can cause a silent rise in pressure? Thats pigmentary glaucoma a rare but treatable form of glaucoma that often goes unnoticed until it starts to affect your vision.
Understanding the Disease
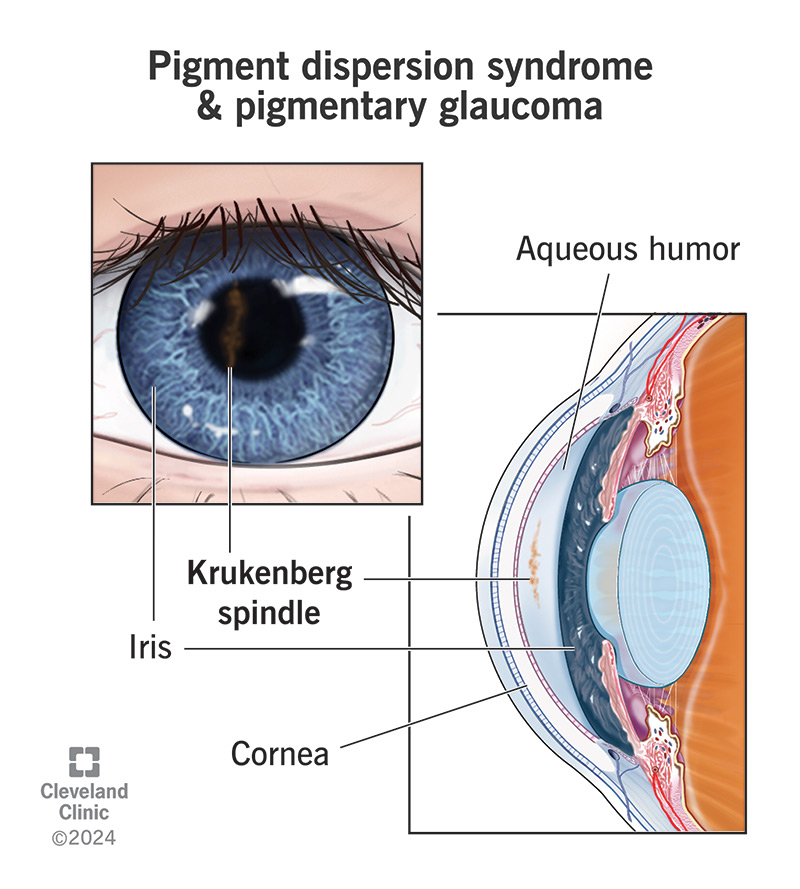
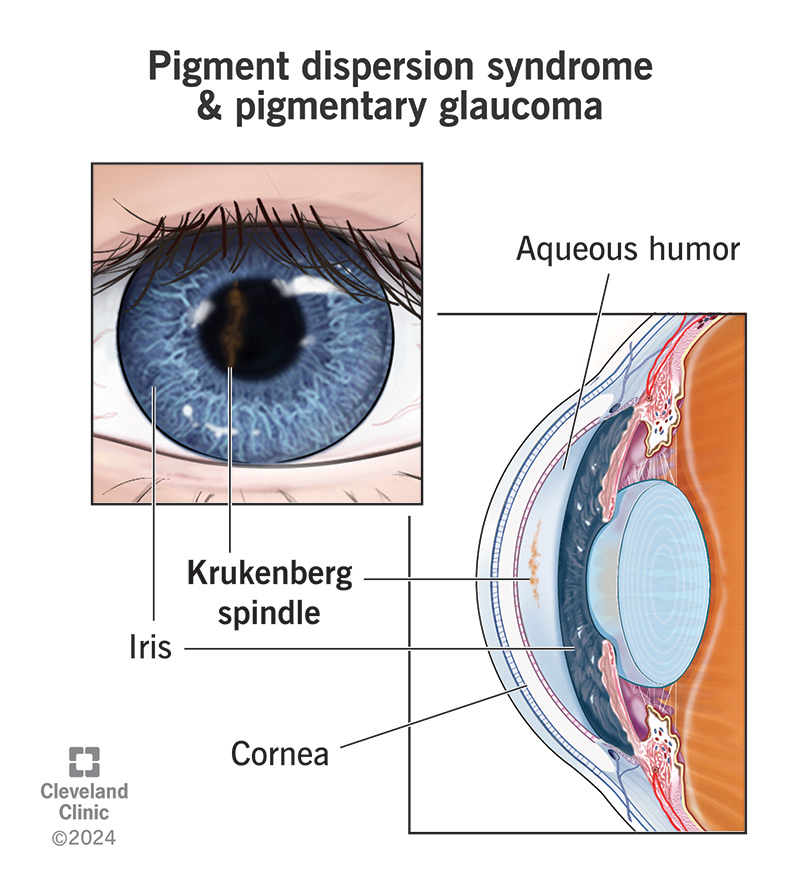
What is pigment dispersion syndrome and how does it turn into pigmentary glaucoma?
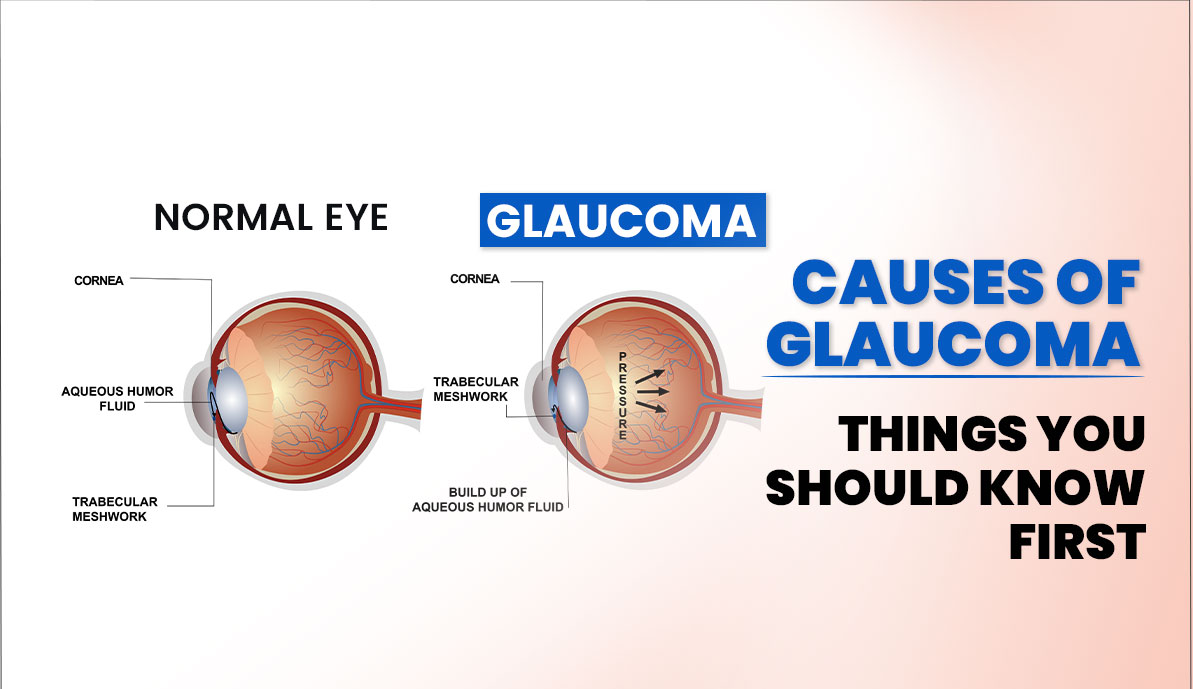
Pigment dispersion syndrome (PDS) is like that one friend who constantly sheds skin cells everywhere. In the eye, tiny pigment granules loosen from the iris and drift into the drainage system (the trabecular meshwork). Over time, this pigment traffic jam blocks fluid outflow, raising intraocular pressure (IOP) and eventually leading to pigmentary glaucoma.
How rare is pigmentary glaucoma?
Its not something youll bump into every day. Studies estimate that pigmentary glaucoma accounts for roughly 0.5%2% of all glaucoma cases, most often affecting young, nearsighted men in their late teens to thirties. So while its uncommon, the impact can be significant if missed.
What are the hallmark symptoms?
Early on, many people notice:
- Intermittent blurry vision or seeing halos around lights.
- A sudden onset of eye redness that seems to come out of nowhere.
- Occasional eye pain that feels more pressure than sting.
As the disease progresses, peripheral vision loss and persistent eye discomfort become more prominent. If you experience any of these, its worth getting an eye examdont brush them off as just fatigue.
What is the longterm prognosis?
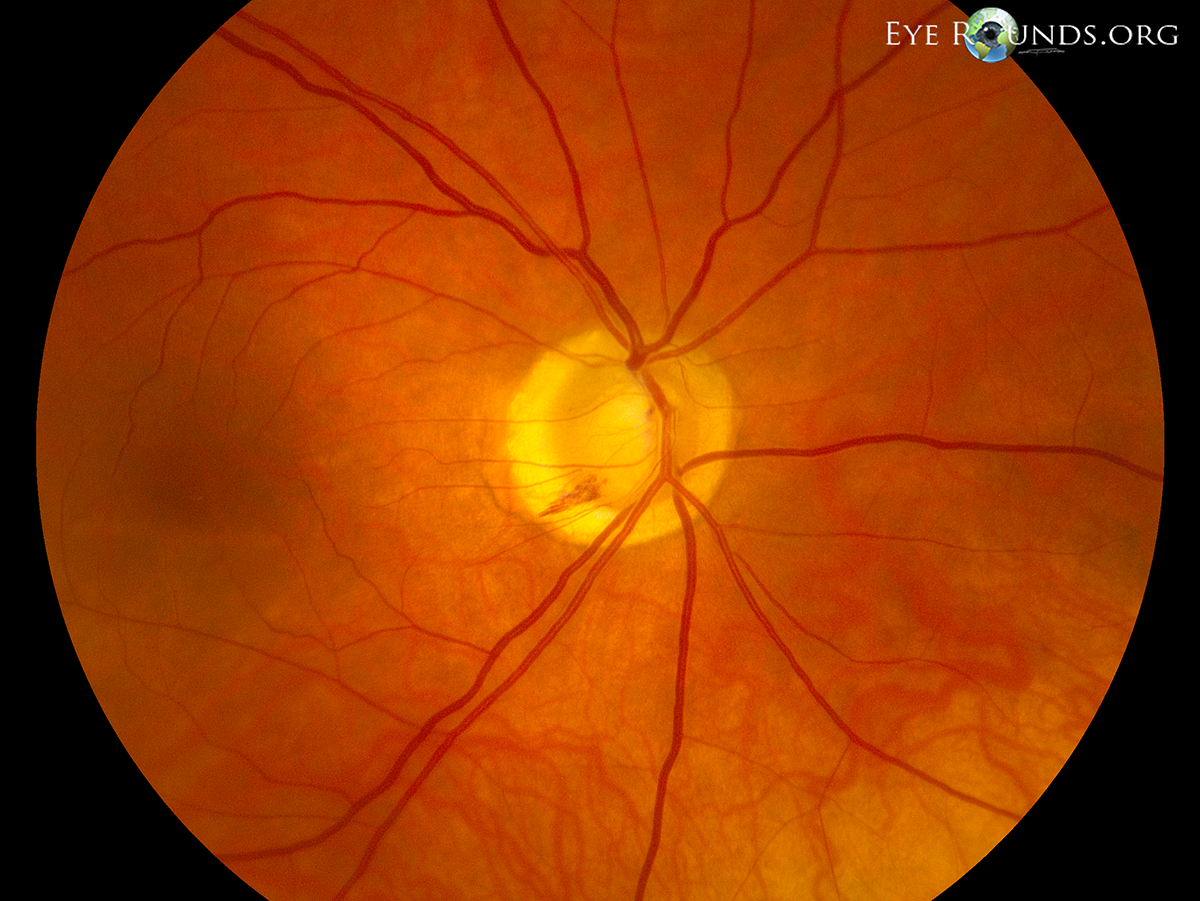
When caught early and managed properly, most patients maintain good visual function for decades. Untreated pigmentary glaucoma, however, can lead to irreversible opticnerve damage and permanent visualfield loss, much like any other form of glaucoma.
How is pigmentary glaucoma coded (ICD10)?
In medical records, the condition is listed under ICD10CM code H40.13. Knowing the code can help you navigate insurance paperwork and ensure you receive the right coverage for treatment.
How It's Diagnosed
Which eyeexam tests are most reliable?
An ophthalmologist will typically run a series of checks:
- Slitlamp exam: Looks for pigment on the corneal endothelium.
- Gonioscopy: Reveals the characteristic Krukenberg spindle a fanshaped pigment pattern on the cornea.
- IOP measurement: Anything over 21mmHg warrants a closer look.
- Optical Coherence Tomography (OCT): Provides a highresolution view of the optic nerve head.
Can a simple home check spot early signs?
While you cant measure IOP at home, you can watch for redeye episodes or sudden halos around headlights at night. If these happen repeatedly, schedule an appointment promptly.
What imaging supports the diagnosis?
Beyond OCT, doctors may use:
- Visualfield testing (Humphrey) to map peripheral vision loss.
- Ultrasound biomicroscopy (UBM) to examine the angle where fluid drains.
Treatment Options Overview
What is the best medical therapy?
Firstline treatment usually starts with prostaglandin analogs (like latanoprost) because they effectively lower IOP with oncedaily dosing. If pressure remains high, doctors may add betablockers, carbonanhydrase inhibitors, or alphaagonists.
| Medication | Typical Effect on IOP | Common Side Effects |
|---|---|---|
| Latanoprost (Prostaglandin) | 25% to 30% | Eye redness, darkening of iris |
| Timolol (Betablocker) | 20% to 25% | Slow heart rate, fatigue |
| Dorzolamide (Carbonanhydrase) | 15% to 20% | Taste disturbance, mild irritation |
When is laser therapy recommended?
If eye drops alone dont keep the pressure in check, laser options step in. , selective laser trabeculoplasty (SLT) offers a safe, repeatable way to boost fluid outflow with minimal downtime.
What surgical routes exist?
When meds and laser fall short, surgeons can consider:
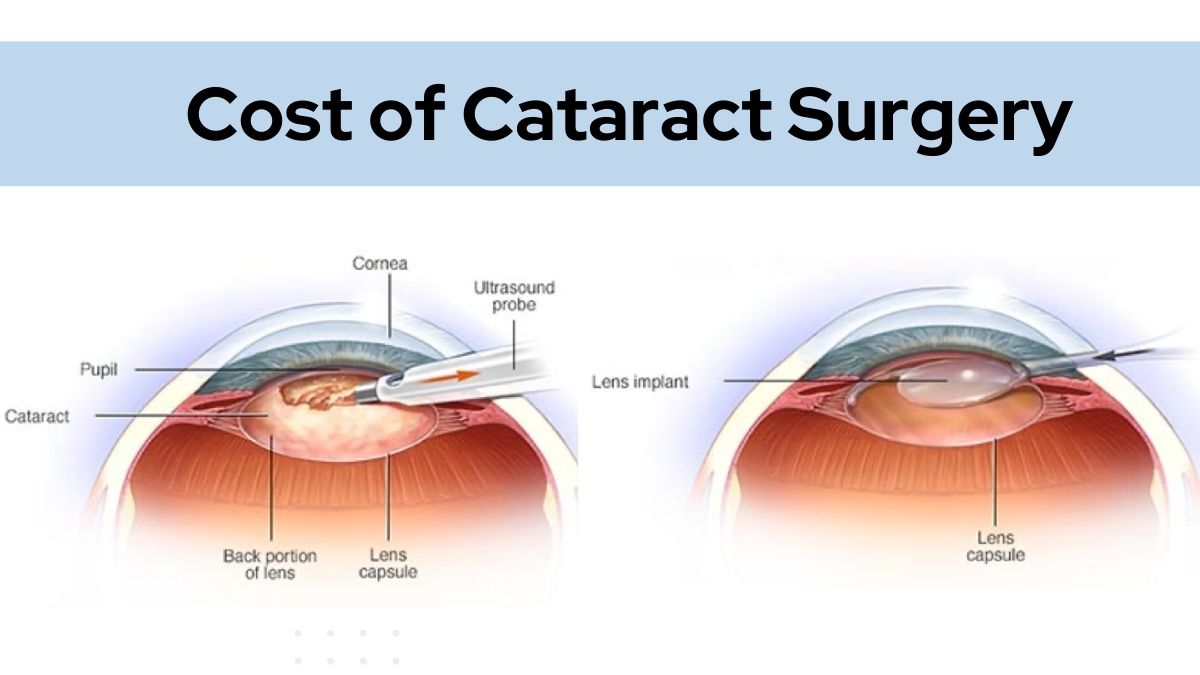
- Trabeculectomy: The goldstandard filtration surgery.
- Glaucoma drainage devices: Ahmed or Baerveldt implants that shunt fluid.
- Minimally invasive glaucoma surgeries (MIGS): iStent or Trabectomesmaller incisions, quicker recovery.
Outcomes vary, but most studies show a 70%80% success rate in achieving target IOP after surgery, especially when combined with postoperative drops.
How do lifestyle tweaks help?
While they wont replace medical care, certain habits can ease the burden:
- Stay active regular aerobic exercise modestly lowers IOP.
- Limit caffeine high caffeine intake can spike pressure temporarily.
- Protect your eyes during sports with polycarbonate lenses.
- Maintain good contactlens hygiene to avoid added irritation.
What followup schedule is typical?
After starting a new regimen, most doctors check IOP monthly for the first six months, then move to quarterly visits. Visualfield tests are usually repeated every 612 months to track any subtle changes.
Balancing Risks & Benefits
What are common treatment complications?
Every option has tradeoffs. Eye drops can cause dryeye or allergic reactions; laser may trigger transient inflammation; surgery carries risks of infection, bleb leaks, or hypotony (too low pressure). Knowing these helps you weigh the pros and cons with your eyecare team.
How to find the sweet spot between benefit and risk?
Think of treatment as a balancing act. A simple riskbenefit matrixlisting each options effectiveness, sideeffects, and recovery timecan turn an overwhelming decision into a clear, stepbystep plan. Your doctor should walk you through it, answering every what if you have.
Can pigmentary glaucoma ever improve on its own?
Spontaneous remission is extremely rare. Even if pressure dips temporarily, the underlying pigment buildup remains, so ongoing monitoring is essential.
How to address the emotional side?
Receiving a glaucoma diagnosis can feel like a punch to the gut. Youre not aloneonline support groups, counseling, and talking openly with friends often lightens the load. Remember, many people live full, active lives with proper management.
RealWorld Perspective
Consider Alex, a 24yearold college student who first noticed halos around streetlights at night. He brushed it off as just tired eyes until a routine eye exam revealed a Krukenberg spindle and an IOP of 28mmHg. His ophthalmologist started latanoprost, added SLT two months later, and Alexs pressure dropped to a safe 15mmHg. Six months on, hes back to studying latenight and playing basketballno longer fearing sudden vision loss.
Stories like Alexs highlight that early detection, combined with a personalized treatment plan, can keep pigmentary glaucoma from stealing your quality of life. If youve experienced similar symptoms, dont waitbook that appointment.
Conclusion
Pigmentary glaucoma may be rare, but its impact is anything but. By recognizing the quirky early signs, understanding how pigment dispersion can clog your eyes drainage, and staying proactive with medication, laser, or surgery, you can protect your vision for the long haul. Keep an eye on your eye health, ask questions, and lean on trusted professionalsyou deserve clear sight and peace of mind. If you have thoughts or personal experiences, share them below; together well navigate this journey.
FAQs
What early signs indicate pigmentary glaucoma?
Typical early clues include intermittent blurry vision, halos around lights, sudden eye redness, and occasional pressure‑type eye pain.
How does pigment dispersion lead to glaucoma?
Pigment granules shed from the iris accumulate in the trabecular meshwork, obstructing fluid outflow and raising intra‑ocular pressure, which can damage the optic nerve.
Which diagnostic tests confirm pigmentary glaucoma?
An eye doctor will perform a slit‑lamp exam, gonioscopy to view pigment on the cornea, IOP measurement, OCT imaging, and visual‑field testing.
What are the first‑line medical treatments?
Prostaglandin analogs such as latanoprost are usually started first, often combined with beta‑blockers or carbon‑anhydrase inhibitors if additional pressure lowering is needed.
When is surgery necessary for pigmentary glaucoma?
Surgery is considered when medications and laser therapy fail to achieve target IOP; options include trabeculectomy, drainage implants, and minimally invasive glaucoma surgeries (MIGS).