What are the first steps to diagnose a pediatric softtissue tumor? Grab a goodquality biopsy, look at the tissue under the microscope, then match the pattern to a list of common childhood lesions.
How can a pathologist tell if a lesion is benign or malignant? By checking cell shape, growth pattern, mitotic activity, and when needed a few stains or a molecular test. Those clues usually point you in the right direction without a lot of guesswork.
First Diagnostic Steps
Imagine you just walked into a lab and a tiny, firm lump from a fiveyearold sits on your slide. Your first instinct is to keep things simple: is it something we can recognize without a fullblown workup? The answer is often yes. Start with a wellfixed, properly oriented specimen freshfrozen tissue for molecular work, plus a formalinfixed piece for routine staining. A clear label and a brief clinical note (age, location, any imaging clues) go a long way toward a speedy diagnosis.
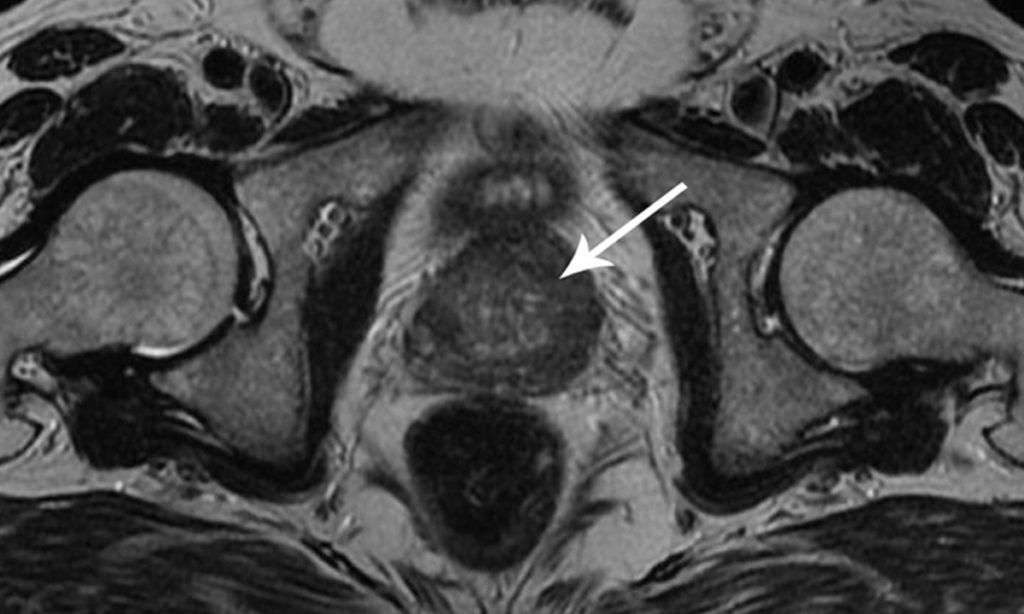
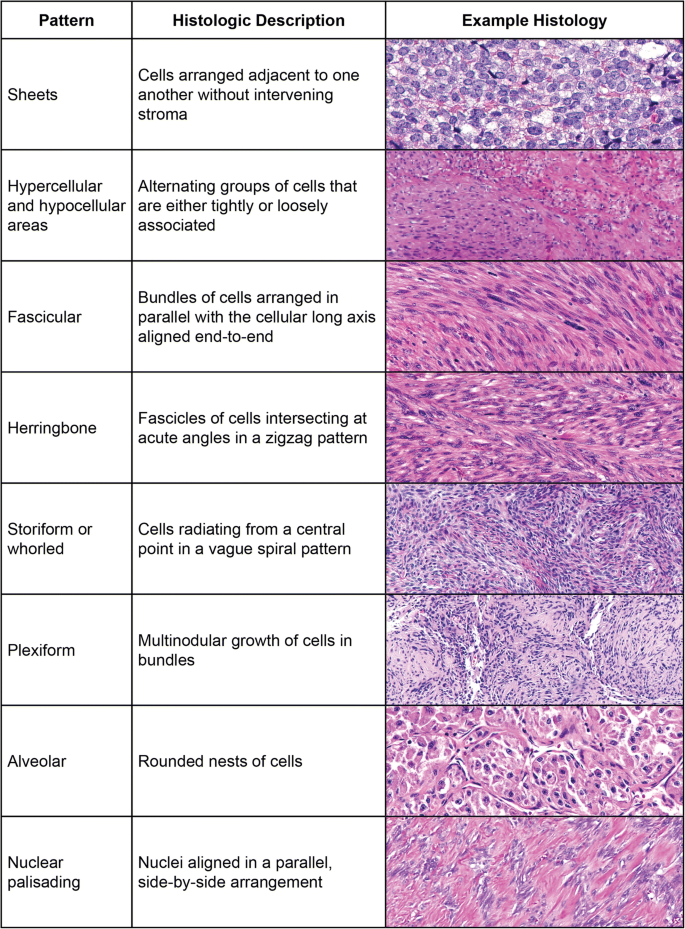
From there, the H&E slide is your canvas. Look for the classic growth patterns that childhood tumors love to flaunt: bundles of spindle cells, nests of round blue cells, or a myxoid (gellike) background. Those visual hints are the stepping stones to the next phase immunohistochemistry (IHC) and, when the picture is fuzzy, molecular testing. For cases where prognosis or post-surgical outlook is a key concern, consider correlating early findings with resources on prostate cancer outlook to practice concise prognostic phrasing in reports and family discussions.
Spectrum of Tumors
Children dont get the same tumor lineup that adults do. Their softtissue masses fall into four broad buckets: malformative, benign, intermediate, and malignant. Knowing which bucket youre in helps you pick the right stains and, later, the right therapy.
Malformative Lesions
Example: Congenital Fibrous Hamartoma of Infancy
This little fellow shows a mix of fibroblasts, fat, and collagen. Its usually painless, appears in the first year of life, and resolves after complete excision. Histology shows a triplecomponent pattern thats unmistakable once youve seen it a few times.
Common Benign Tumors
Quick List
- Infantile fibromatosis long fascicles of bland spindle cells.
- Lipoblastoma lobulated fat with myxoid septa.
- Dermatofibrosarcoma protuberans (lowgrade) storiform spindle cells.
- Myofibroma biphasic pattern with hemangiopericytomalike vessels.
- Granular cell tumor polygonal cells full of PASpositive granules.
Intermediate / LowGrade Tumors
Comparison Table
| Entity | Typical Age | Location | Key Genetic Alteration |
|---|---|---|---|
| Myxoid LM | 38y | Extremities | None specific |
| Lowgrade Fibromyxoid Sarcoma | Teenagers | Deep soft tissue | FUSCREB3L2 fusion |
Malignant Sarcomas that Dominate
Top Five
- Rhabdomyosarcoma alveolar or embryonal, MyoD1 & Myogenin positive.
- Infantile Fibrosarcoma ETV6NTRK3 fusion, often in the extremities.
- Ewing Family Tumors CD99 membranous staining, EWSR1FLI1 fusion.
- Undifferentiated Sarcoma high mitotic rate, no lineage specific marker.
- Alveolar SoftPart Sarcoma TFE3 nuclear positivity, rare in kids.
Each of these entities carries its own set of redflag features, and the good news is that most can be confirmed with a targeted panel of IHC stains and a quick molecular test.
StepbyStep Algorithm
When you feel a little lost, think of the diagnostic pathway as a staircase. One step at a time, youll get from a lump to a definitive label.
Optimal Tissue Handling
Checklist
- Freshfrozen core for RNAbased assays.
- Formalinfixed paraffinembedded (FFPE) block for H&E and IHC.
- Avoid decalcification unless bone is involved.
- Label every slide with patient age, site, and clinical impression.
Histologic Clues to Look For First
FlowChart
- Growth pattern fascicular, storiform, nests?
- Cell type spindle, round, epithelioid?
- Stroma collagenous, myxoid, hyalinized?
- Mitotic activity rare, moderate, brisk?
When to Apply Immunohistochemistry
Decision Tree
If the morphology suggests a spindlecell lesion, start with a panel of Desmin, SMA, Myogenin, S100, CD99, and Ki67. For roundcell tumors, add TTF1, CD45, and NKX22. The pattern of positivity will usually narrow the field to one or two possibilities.
Molecular Testing Essentials
Key Fusions & Platforms
- ETV6NTRK3 (Infantile Fibrosarcoma) RTPCR or targeted NGS.
- FUSCREB3L2 (Lowgrade Fibromyxoid Sarcoma) FISH or NGS.
- EWSR1FLI1 (Ewing) FISH is fast and reliable.
- MYOD1 L122R (Sclerosing Rhabdomyosarcoma) Sanger sequencing.
Integrating Radiology
Quick Reference
Imaging can clue you in on depth, vascularity, and bone involvement. According to the , MRI is the workhorse for softtissue masses, while CT helps when you suspect calcifications or lung metastases.
Pediatric Mass Differential
If youve ever stared at a spindlecell tumor under the microscope and felt the whatnow? moment, youre not alone. The differential list can be long, but a systematic approach trims it down fast.
Infantile Fibrosarcoma vs. FibrosarcomaLike Lesions
Comparative Table
| Feature | Infantile Fibrosarcoma | FibrosarcomaLike Lesion |
|---|---|---|
| Age | 02y | Older children |
| Location | Extremities | Deep trunk |
| Genetics | ETV6NTRK3 | None specific |
| IHC | Vimentin+ | Vimentin+ |
Rhabdomyosarcoma LookAlikes
Key Distinguishers
- Alveolar SoftPart Sarcoma strong nuclear TFE3, granular cytoplasm.
- Desmoplastic Small Round Cell Tumor WT1 (Cterminal) positivity.
- Clear Cell Sarcoma S100 plus melanocytic markers (HMB45).
When Tumor of Uncertain Origin Appears
ThreePoint Checklist
- Reexamine H&E with a second pathologist.
- Run a broad IHC panel (panCK, S100, Desmin, CD34).
- Consider RNAbased sequencing for novel fusions.
Using Pediatric Tumors Pathology Outlines
Helpful Resource
For a readymade cheatsheet that lists the most common entities, their histology, and recommended stains, see the page. Its a favorite reference for many trainees and seasoned pathologists alike.
Modern Molecular Tools
The age of eyeballing a tumor is over not because microscopes are old school, but because genetics can give you a crystalclear answer when morphology is ambiguous.
Standard Molecular Assays
Whats on the Menu?
- NTRK testing (immunostain, FISH, or NGS) essential for infantile fibrosarcoma.
- ALK rearrangements rare but actionable in some spindlecell sarcomas.
- MYOD1 L122R mutation signals a poorer prognosis in rhabdomyosarcoma.
- SMARCB1 (INI1) loss points to malignant rhabdoid tumor.
AIAssisted Pathology
Is a Robot Helping?
Recent studies show deeplearning algorithms can flag subtle nuclear atypia and suggest likely diagnoses in seconds. While AI isnt replacing the human eye, it can prioritize cases that need urgent review a handy safety net for busy pediatric labs.
Dealing with Ambiguous Results
GrayZone Flowchart
- Result positive for a known fusion? Report and recommend targeted therapy.
- Result negative but morphology suspicious? Recommend broader NGS panel.
- Result equivocal? Seek a second opinion from a pediatric sarcoma reference center.
Quick FAQ Answers
Is a biopsy always required? Almost always, because imaging alone cant tell you the exact tumor type.
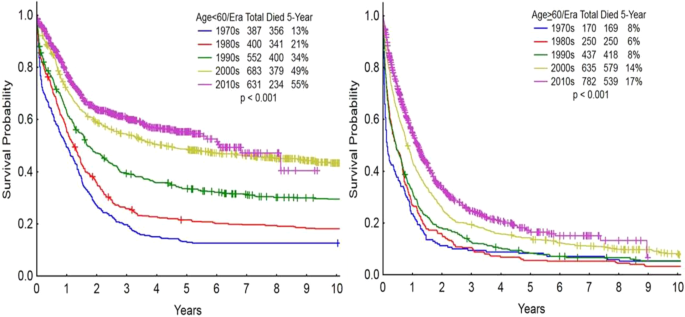
Whats the prognosis for infantile fibrosarcoma after complete resection? Over 90% longterm survival when the tumor is fully removed, especially if the ETV6NTRK3 fusion is present.
How often do pediatric softtissue tumors recur? Recurrence rates vary: benign lesions <5%, intermediate 1020%, malignant up to 4050% depending on margins and biology.
What redflag histologic features demand urgent reporting? High mitotic index, necrosis, marked pleomorphism, and any evidence of vascular invasion.
Practical Takeaways
SpecimenSubmission Checklist
- Fresh frozen core for RNA/NGS.
- FFPE block with at least two H&E sections.
- Clinical note: age, site, imaging impression.
- Label Pediatric Soft Tissue Tumor clearly.
IHC & Molecular CheatSheet
- Spindle cells SMA, Desmin, S100, CD34.
- Round cells Myogenin, MyoD1, CD99, NKX22.
- Key fusions ETV6NTRK3, FUSCREB3L2, EWSR1FLI1.
Communication with Oncology
- State clearly if the lesion is benign, intermediate, or malignant.
- Include any actionable molecular findings (e.g., NTRK fusion).
- Suggest next steps: complete resection, referral to a sarcoma center, or targeted therapy trial.
Trusted Resources
Guidelines & Classifications
The WHO 2024 SoftTissue Tumor Classification remains the gold standard for nomenclature and diagnostic criteria. Its freely available through most academic libraries.
OpenAccess Textbooks & Slides
AMP.org offers a slidedeck on pediatric softtissue sarcoma that walks you through each entity with realworld images. Its a great visual companion to the text youre reading now.
PeerReviewed Articles for Deep Dives
Key papers youll want to bookmark include the Allen Press review on pediatric sarcoma pathology, the PubMed series on molecular diagnostics, and the recent ScienceDirect article on morphomolecular integration in childhood tumors. For clinicians writing familyfacing material, review examples of clear prognostic language such as those found in articles about survival without prostate to practice balancing hope with realistic expectations.
Conclusion
Diagnosing pediatric softtissue tumors is a blend of art and science. By following a systematic algorithm, using the right stains, and leaning on modern molecular tools, you can turn a puzzling mass into a clear diagnosis that guides precise treatment. Remember, every case is an opportunity to balance the benefits of early, accurate labeling with the risks of overtesting a careful, compassionate approach builds trust with families and ensures the best outcomes. If youre navigating a confusing case, grab the cheatsheet, check the guidelines, and dont hesitate to reach out to a pediatric sarcoma specialist. Together, we can make sure every child gets the right answer at the right time.
FAQs
What is the first step in diagnosing pediatric soft tissue tumors?
A biopsy is essential for diagnosis, followed by microscopic examination and immunohistochemistry to classify the tumor.
How do pathologists distinguish benign from malignant pediatric soft tissue tumors?
Pathologists assess cell shape, growth pattern, mitotic activity, and use special stains or molecular tests to determine tumor behavior.
Which pediatric soft tissue tumors are most common?
Rhabdomyosarcoma is the most common, followed by infantile fibrosarcoma and other sarcomas like Ewing family tumors.
What molecular tests are important in pediatric soft tissue tumor pathology?
Key tests include ETV6-NTRK3 for infantile fibrosarcoma, FUS-CREB3L2 for low-grade fibromyxoid sarcoma, and EWSR1-FLI1 for Ewing tumors.
What are the main histologic features of pediatric soft tissue tumors?
Common features include spindle cells, round blue cells, myxoid stroma, and specific growth patterns that help guide diagnosis.