Most people dont realize that a childs complaint of chest pain can be a puzzle thats both simple and, at times, serious. Below youll find a friendly, stepbystep pediatric chest pain algorithm that cuts through the confusion, so you can decide when to watch, when to test, and when to call in a specialistwithout drowning in unnecessary paperwork.
Think of this as a chat over coffee with a colleague whos been there: youll get the fasttrack answers you need, plus a few realworld stories that show why each step matters.
Why It Matters
What makes pediatric chest pain different?
Kids arent just small adults. Their bodies handle pain, stress, and disease differently, and the causes of chest pain often sit on the opposite end of the spectrum. While adults worry about heart attacks, children are more likely to be dealing with muscle strains, growthrelated soreness, or a lingering cough.
How often is it serious?
Studies show that less than5% of chest pain cases in children are cardiac in origin, while over90% are musculoskeletal or benign respiratory issues. Thats why a solid pediatric chest pain workup is essentialto catch the rare red flags early without overtesting the rest.
Key Statistics
| Cause | Approximate Frequency |
|---|---|
| Musculoskeletal | ~55% |
| Respiratory (pleuritic, asthma) | ~30% |
| Gastroesophageal reflux | ~10% |
| Cardiac (pericarditis, myocarditis, arrhythmia) | <5% |
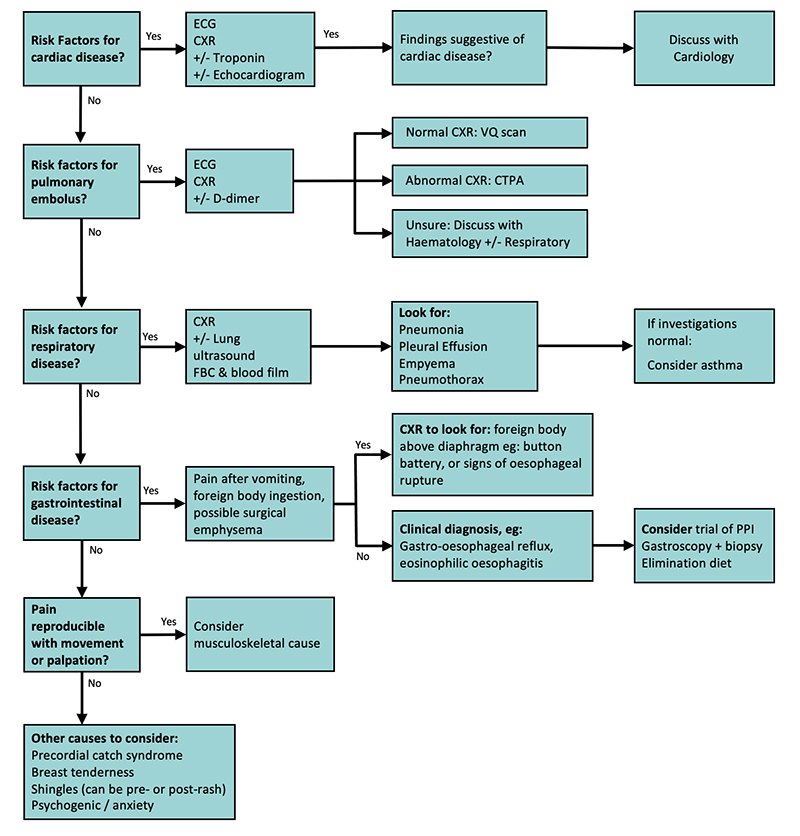
Algorithm Overview
Onepage flowchart
For a quick visual, download the . It walks you through the decision tree in less than a minute.
Core decision nodes
The algorithm hinges on three pillars:
- Redflag screening look for danger signs like severe dyspnea, syncope, or abnormal vitals.
- Initial examination a focused history and physical.
- Tiered testing start with ECG and basic labs for lowrisk kids; move to echo or Holter only if the red flags appear.
RedFlag vs LowRisk Checklist
| RedFlag Signs | LowRisk Indicators |
|---|---|
| Tachycardia >130 bpm (ageadjusted) | Normal heart rate and blood pressure |
| Syncope or nearsyncope | Stable vitals, no syncope |
| Chest pain worsens with exertion | Pain unrelated to activity |
| Fever >38C with chest pain | Aspiration of pain, no fever |
| Murmur or abnormal lung sounds | Normal cardiac and pulmonary exam |
StepbyStep Workup
History & Physical
Ask simple, openended questions: When did the pain start? Can you point to it? Does anything make it better or worse? Kids often describe pain as sharp, stabbing, or hurting like a bruise. Note associated symptomscough, fever, shortness of breath, or gastrointestinal upset.
Sample script for a 10yearold
Hey, Im Dr. Sam. Can you tell me where it hurts? Does it feel like a pinch or more like a sore muscle after soccer? Using their own words makes the exam feel less clinical.
RedFlag Screening (MDM)
Run through the checklist above. If any red flag pops up, treat it as a stopandthink momentthis is where the pediatric chest pain mdm (medical decisionmaking) kicks in.
Tier1 Tests for LowRisk Patients
- ECG often normal, but a quick way to rule out arrhythmia.
- Basic labs CBC and BMP; look for infection or electrolyte shifts.
- Chest Xray only if the exam hints at lung involvement (e.g., wheeze, pleuritic pain).
When to skip the ECG
If the child has a completely benign exam, normal vitals, and no redflag symptoms, you can safely defer the ECG and focus on reassurance.
Tier2 Cardiac Testing (IntermediateRisk)
When something feels offan abnormal ECG, murmurs, or persistent painmove to more detailed studies:
- Echocardiogram visualizes pericardial effusion, structural abnormalities.
- Holter monitor catches intermittent arrhythmias.
- Cardiac MRI (rarely) for suspected myocarditis when echo is inconclusive.
Echocardiogram vs. Holter vs. Event Monitor
| Test | Best For | When to Use |
|---|---|---|
| Echocardiogram | Structural disease, pericardial effusion | Abnormal heart sounds, persistent pain, suspicion of pericarditis |
| Holter (2448h) | Frequent arrhythmias | Palpitations, irregular pulse on exam |
| Event monitor (up to 30d) | Rare, symptomatic episodes | Syncope with no ECG changes |
Referral Criteria
If you suspect any of the following, call pediatric cardiology right away:
- Signs of pericarditis (pericardial rub, fever, ECG changes) see the .
- Myocarditis suspicion (chest pain + elevated troponin) follow the .
- Persistent unexplained tachyarrhythmia.
- Structural heart disease identified on echo.
Common Causes
Musculoskeletal
Think growing pains or an overuse injury after sports. The exam usually reveals reproducible tenderness and a normal cardiac workup. Reassure the family, prescribe a short course of NSAIDs, and advise gentle stretching.
Reassurance script
Your childs heart is fine; the pain is most likely from sore muscles that happened after soccer practice. A few days of rest and ibuprofen should do the trick.
Pleural or Pulmonary
Pleuritic chest pain often comes with a cough or fever. A quick chest Xray can spot pneumonia or a small effusion. Treat the infection, and the pain usually fades within a week.
Gastroesophageal Reflux
Acid can irritate the esophagus, mimicking heart pain. A trial of a protonpump inhibitor (PPI) for 24weeks can be both diagnostic and therapeutic.
Psychogenic / Functional Pain
Anxiety, stress, or even school pressures can manifest as pain that has no physical cause. Screening tools like the PHQ9 or GAD7 help identify underlying anxiety, and a brief talk with a mentalhealth professional often brings relief.
Cardiac (Pericarditis, Myocarditis, Arrhythmia)
These are the rare but serious culprits. Look for fever, a pericardial rub, or abnormal ECG changes. Early echo and cardiology input make the difference between a quick recovery and a prolonged hospital stay.
Institution Pathways
JohnsHopkins Pathway
The JohnsHopkins chest pain clinical pathway emphasizes early redflag detection and recommends a single ECG for any child with abnormal vitals. The PDF is a handy bedside reference.
CHOP Pathway
CHOPs algorithm adds an efficiency layer: if the ECG is normal and the exam shows no murmur, the child can be discharged with a returnifworse instruction sheet.
RCH Chest Pain Pathway
RCH (Royal Childrens Hospital, Melbourne) incorporates a brief observation period (30min) for lowrisk kids before discharge, reducing unnecessary imaging.
PrintReady Pocket Card
Consider creating a laminated pocket card that lists redflag symptoms, the basic workup steps, and direct phone numbers for cardiology. Its a small tool that saves big time.
FAQs (FeaturedSnippet Ready)
When is chest pain in a child an emergency?
If the child shows any redflag signsevere shortness of breath, fainting, strikingly fast heart rate, or a new murmurtreat it as an emergency and call cardiology immediately.
Do I need an ECG for every child with chest pain?
No. For a child with a normal exam, stable vitals, and no red flags, an ECG can often be skipped. The algorithm helps you decide when its truly necessary.
How many children actually need a cardiac workup?
Less than5% of cases end up needing detailed cardiac testing. Thats why a focused redflag screen saves both families and clinicians from unnecessary stress.
Whats the difference between pericarditis and myocarditis?
Pericarditis inflames the sac around the heart, often causing sharp pain that improves when leaning forward. Myocarditis involves the heart muscle itself and may present with fatigue, shortness of breath, or elevated troponin. Both require cardiology followup.
Can anxiety cause chest pain?
Absolutely. Stress can tighten chest muscles and create a sensation of pain. A calm conversation, breathing exercises, and possibly a mentalhealth referral can resolve it.
RealWorld Cases
CaseA: LowRisk Soccer Injury
Alex, 12, complained of a dull ache after a football game. Vitals were normal, the pain reproduced when pressing the left pectoral muscle, and the ECG was flat. The algorithm guided the team to skip imaging, prescribe ibuprofen, and send Alex home with a stretching plan. He was painfree in three days.
CaseB: FeverDriven Pericarditis
Lila, 8, presented with a fever of 38.7C and a sharp chest pain that worsened when she sat up. The exam revealed a pericardial rub. The redflag screen prompted an immediate ECG (diffuse ST elevation) and an echo that showed a small pericardial effusion. Following the pediatric pericarditis guidelines, she received NSAIDs and was monitored for 48hours. She recovered fully.
CaseC: AnxietyRelated Pain
Sam, 15, reported intermittent chest pressure during exams. All vitals, ECG, and labs were normal. A PHQ9 screened positive for moderate anxiety. The algorithm led the clinician to a brief counseling session and a referral to the school psychologist. Within a month, Sams chest discomfort resolved.
Lesson
These stories highlight how the pediatric chest pain algorithm balances safety (catching the rare serious cases) with practicality (avoiding needless tests).
Resources & Downloads
Downloadable PDF
Grab the full to keep on your desk or EMR sidebar.
Key Guidelines
- American Academy of Pediatrics (AAP) review on chest pain in children.
- ESC guidelines for pericardial disease.
- Recent SCAMP study (2023) on emergency department outcomes.
Quick Reference Chart
Print a onepage chart that lists redflag symptoms, the basic workup sequence, and the phone number for your oncall pediatric cardiology team.
Balancing Benefits & Risks
Benefits
Implementing the algorithm reduces unnecessary radiation, cuts down on costly imaging, and shortens ED staysallowing families to return home sooner with confidence.
Risks
The only real risk is missing a subtle cardiac issue. Thats why the redflag step acts as a safety net: if anything feels off, you pause, reassess, and consider higherlevel testing.
SafetyNet Tips
- Reevaluate in 2448hours if pain persists despite a lowrisk workup.
- Educate parents on warning signsworsening pain, new shortness of breath, or fainting.
- Document the decisionmaking process thoroughly (helps both the team and medicolegal review).
Conclusion
Navigating chest pain in kids doesnt have to be a guessing game. By following a clear pediatric chest pain algorithm, you can swiftly separate the harmless from the potentially lifethreatening, sparing families unnecessary tests while still catching the rare serious conditions. Download the printable pathway, keep the redflag checklist visible, and trust your clinical instinctsbecause youre the best advocate for your little patients.
Whats your experience with pediatric chest pain? Have you found a particular tip especially helpful? Share your thoughts in the comments, and feel free to ask any questionsyoure not alone on this journey.
For caregivers worried about recurrent or exerciseassociated chest pain, review guidance on pediatric chest pain to compare symptom descriptions and recommended followup.
FAQs
What are the most common red‑flag signs in pediatric chest pain?
Red‑flags include tachycardia >130 bpm (age‑adjusted), syncope or near‑syncope, chest pain worsened by exertion, fever >38 °C with pain, and new murmurs or abnormal lung sounds.
Do all children with chest pain need an ECG?
No. An ECG is recommended only if the child has abnormal vitals, a red‑flag symptom, or a concerning physical exam. Low‑risk patients with a normal exam can be safely discharged without an ECG.
When should I refer a child to pediatric cardiology?
Refer immediately if there are signs of pericarditis, myocarditis (elevated troponin or abnormal echo), unexplained tachyarrhythmia, or structural heart disease identified on imaging.
Can anxiety cause chest pain in kids, and how should it be managed?
Yes. Stress or anxiety can produce functional chest discomfort. Screening tools like the PHQ‑9 or GAD‑7 help identify anxiety, and a brief counseling session with a mental‑health referral often resolves the pain.
What is the typical work‑up for a low‑risk child with chest pain?
For low‑risk patients, the algorithm recommends a focused history, physical exam, and possibly basic labs (CBC, BMP). An ECG and chest X‑ray are reserved for cases with any red‑flag findings.