Spotting a cloudy spot in a childs eye can feel like an alarm bell ringing in the middle of a quiet night. A pediatric cataract is that cloudy spot often appearing as a milkygray patch or a white pupil and it can show up when you least expect it. If you catch it early, simple steps and timely treatment can keep your little ones vision bright. If you wait, the damage can become permanent. Below is the fasttrack guide that answers the biggest questions, walks you through the Rule of 7, explains the different types, and shows exactly what to expect before, during, and after surgery.
Quick Facts
What is the Rule of 7 in pediatric cataract?
The Rule of 7 is a handy checklist of seven warning signs that parents can watch for during routine checkups or at home. Its called a rule because catching any one of these signs early can trigger a prompt eye exam, dramatically improving outcomes.
How do I use it with my child?
Keep an eye out for these clues:
| Sign | Typical Age | What to Do |
|---|---|---|
| White or milky pupil | Birthto2years | Schedule an eye exam ASAP |
| Sudden eye turning (strabismus) | 6months3years | Ask pediatrician for a referral |
| Cloudy vision in photographs | Any age | Ask for a specialist consultation |
| Excessive tearing or photophobia | Infancyearly childhood | Book a comprehensive eye exam |
| Red reflex absent on flashlight | Newborn1year | Urgent ophthalmology referral |
| Developmental delays in visual milestones | 012months | Early vision screening |
| Frequent eye rubbing | Toddlerpreschool | Check for underlying cataract |
Why is this rule vital?
Because a childs visual system is most plastic in the first few years. The sooner you intervene, the better the brain can adapt, reducing the risk of amblyopia (also called lazy eye).
Types Explained
What are the main pediatric cataract types?
Broadly, cataracts in kids fall into two camps:
- Congenital cataract: Present at birth or diagnosed within the first few weeks.
- Acquired cataract: Develops later, often due to injury, infection, or metabolic issues.
How do morphologic classifications differ?
Doctors also look at where the cloudiness sits inside the lens. Common morphologies include:
- Lamellar a layered opacity.
- Nuclear clouding in the central core.
- Posterior subcapsular a plate right behind the lens capsule.
When does juvenile cataract typically appear?
Juvenile cataract usually refers to cases emerging between age5 and 12 (often called schoolage cataract). These often have an inherited component or are linked to systemic diseases.
Comparison of Types
| Type | Etiology | Visual Impact | Typical Treatment |
|---|---|---|---|
| Congenital | Genetic, TORCH infections | Severe, threatens development | Surgery + aphakic correction |
| Acquired (trauma) | Physical injury | Variable, often unilateral | Surgery, possible IOL |
| Acquired (metabolic) | Diabetes, galactosemia | Gradual clouding | Treat underlying disease + surgery |
Why It Happens
Which genetic factors cause cataracts?
Mutations in genes like CRYAA and GJA8 are common culprits. Families with a history of lens opacities often undergo genetic counseling to understand recurrence risk.
Can infections lead to pediatric cataract?
Yes. Inutero infections known as TORCH (Toxoplasmosis, Others, Rubella, Cytomegalovirus, Herpes) can damage the developing lens. Prompt maternal screening and treatment can reduce the odds of cataract formation.
What metabolic disorders are linked?
Conditions such as galactosemia, diabetes, and certain storage diseases can cause the lens to swell and become opaque. Managing the systemic disease is a critical piece of the treatment puzzle.
How does trauma trigger cataracts?
A blunt or penetrating eye injury can break the lens fibers, leading to opacification. Even seemingly minor bumps can sneakily lead to a cataract months later.
Realworld vignette
Imagine a 3monthold named Maya. Her pediatrician noticed a white reflex in a routine photoscreen, but Mayas parents thought it was just a reflection. A quick referral to a pediatric ophthalmologist confirmed a congenital cataract. Thanks to the Rule of 7 awareness, Mayas surgery happened at 6weeks, preserving her visual potential. After surgery, careful monitoring for issues like dry eye disease during recovery helped keep her comfortable as vision therapy began.
Treatment Options
When is surgery absolutely necessary?
Any cataract that blocks the visual axis (the clear line of sight) or causes significant refractive error demands surgery, especially before 6months of age when the visual system is rapidly developing.
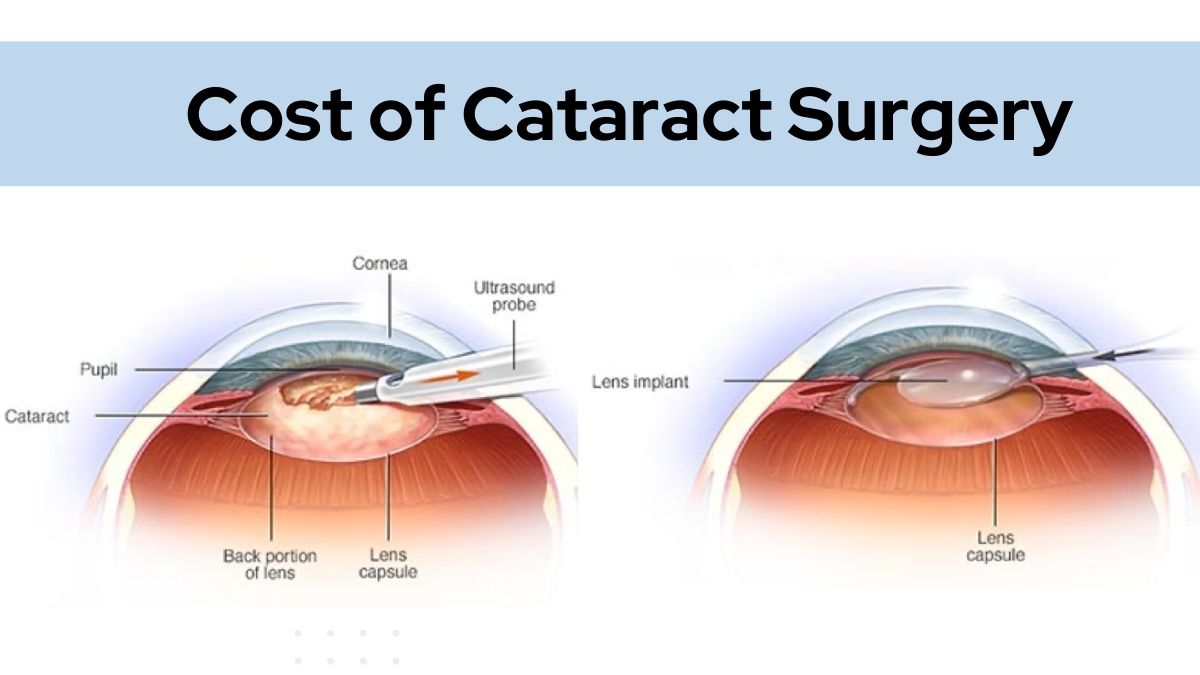
What does pediatric cataract surgery involve?
Modern surgery typically includes:
- Lens removal via a tiny incision.
- Vitrectomy (removing the front vitreous) to prevent posterior capsule opacification.
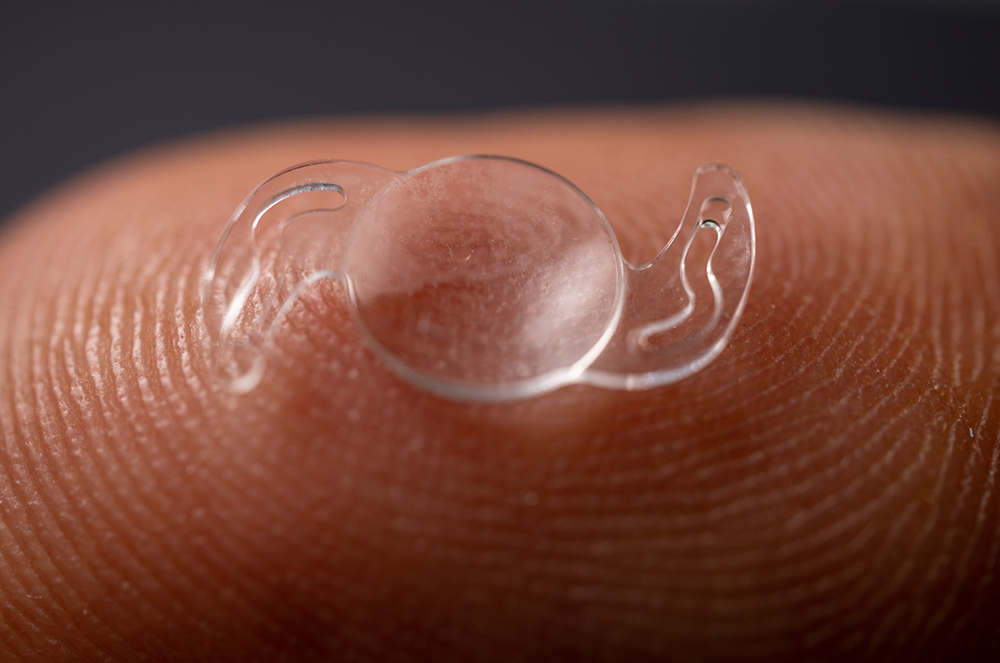
- Optional primary intraocular lens (IOL) implantation decided based on age, eye size, and future growth.
According to , success rates for visual improvement exceed 80% when performed early.
What about nonsurgical treatments?
When surgery isnt immediately feasible (e.g., extremely low birth weight infants), doctors may fit the child with a contact lens or aphakic glasses to focus light correctly. Simultaneously, amblyopia therapyoften patching the stronger eyehelps train the brain to use the operated eye.
Stepbystep surgery day
- Preop checklist: Blood work, anesthesia clearance, fasting.
- Anesthesia: General anesthesia ensures no movement.
- Procedure: Tiny instruments remove the cloudy lens; surgeon may place an IOL.
- Recovery: A few hours of monitoring, then discharge with eye drops.
- Followup: First visit within 2448hours, then weekly to monitor healing.
Risks & Benefits
What are the biggest benefits?
Early surgery can:
- Restore clear vision, allowing normal visual development.
- Prevent amblyopia, giving the child a chance at 20/20 vision.
- Reduce the need for lifelong glasses or contacts if an IOL is placed.
Which complications should I watch for?
While rare, the following can occur:
- Posterior capsule opacification (PCO): A secondary cataract that may need a quick laser treatment.
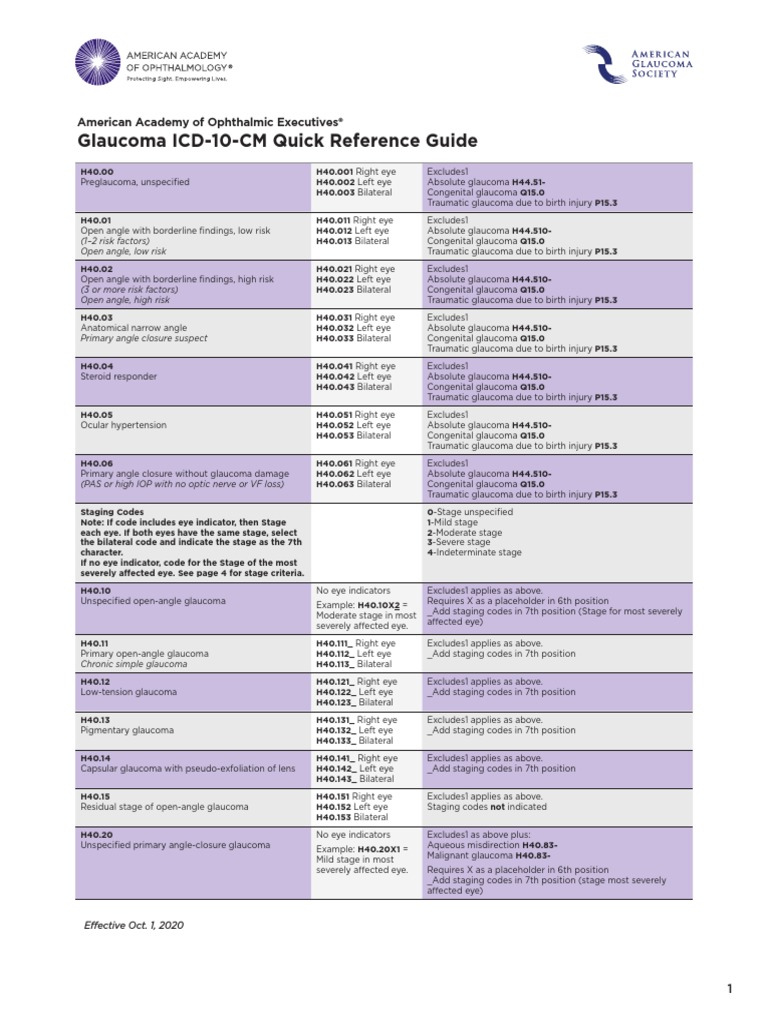
- Glaucoma: Increased eye pressure developing months to years later.
- Retinal detachment: Very uncommon but serious.
- Infection (endophthalmitis): Prompt antibiotic eye drops reduce risk.
RiskBenefit Matrix
| Benefit | Potential Risk | Mitigation Strategy |
|---|---|---|
| Clear vision | PCO | Regular laser capsulotomy if needed |
| Reduced amblyopia | Glaucoma | Longterm IOP monitoring |
| Potential IOL use | Retinal detachment | Surgeon expertise, vigilant followup |
After Surgery
What does immediate postop care look like?
Parents will be instructed to administer antibiotic and antiinflammatory eye drops several times a day. A protective shield may be placed over the eye while sleeping for the first week.
How does amblyopia therapy fit in?
Even after a clear lens, the brain may have ignored the eye for months. Patching the stronger eye for a few hours each day forces the brain to use the operated eye, strengthening its visual pathways. Success often hinges on consistencythink of it like daily exercise for the eye.
What longterm monitoring is needed?
Children will need routine exams at 1month, 3months, 6months, and then annually. These visits check for:
- Intraocular pressure (glaucoma screening).
- Refractive changes as the eye grows.
- Stability of any implanted IOL.
FAQ QuickFire (Featured SnippetReady)
- Can a child outgrow a pediatric cataract? Nocataracts dont resolve spontaneously; they require medical intervention.
- How long is recovery? Most children resume normal activities within 12 weeks; visual acuity continues to improve over months with therapy.
- Do all kids need glasses after surgery? Not alwaysif a primary IOL is placed and the eye grows predictably, glasses may be unnecessary, but many still need occasional prescription updates.
Helpful Resources
Where can I find trustworthy information?
Start with reputable sites such as the , , and the American Academy of Ophthalmologys fact sheets. They keep the data uptodate and cite peerreviewed studies.
How do I choose a pediatric ophthalmologist?
Look for board certification in pediatric ophthalmology, years of experience with infant cataract surgery, and positive patient reviews that mention bedside manner and postop support. A quick phone call to ask about their volume of pediatric cases can give you confidence.
Are there community groups for support?
National organizations such as the host parent forums, and many hospitals have local support circles. SlideShare presentations titled Pediatric Cataract Management often include valuable visual guides you can download for free.
Conclusion
Seeing a white or cloudy pupil in your child can be terrifying, but armed with the Rule of 7, knowledge of the different cataract types, and a clear roadmap for treatment, you can turn that fear into action. Early surgery, diligent followup, and consistent amblyopia therapy give your child the best chance at a bright visual future. If you suspect anything unusual, dont waitschedule an eye exam, reach out to a trusted pediatric ophthalmologist, and lean on the reputable resources listed above. Your childs eyes deserve every ounce of care, love, and attention you can give.
FAQs
What are the first signs of pediatric cataract?
Look for a white or milky pupil, abnormal eye turning (strabismus), excessive tearing, photophobia, or a missing red reflex during a flashlight exam.
When should surgery be performed for a child with cataract?
Any cataract that blocks the visual axis or causes significant refractive error should be removed, preferably before 6 months of age for optimal visual development.
Can a child outgrow a cataract without treatment?
No. Cataracts do not resolve on their own; they require medical or surgical intervention to prevent permanent vision loss.
What is amblyopia therapy and why is it needed after cataract surgery?
Amblyopia therapy (often patching the stronger eye) forces the brain to use the operated eye, helping it develop normal visual pathways after surgery.
How often should my child be followed up after pediatric cataract surgery?
Typical follow‑up visits are at 1 month, 3 months, 6 months, and then annually to monitor intra‑ocular pressure, refractive changes, and lens stability.