Finding out you have proliferative diabetic retinopathy (PDR) feels a lot like hearing your favorite song is on the radioonly youre not sure if the tune will end well. The good news? There are proven ways to protect your sight, and each comes with its own tradeoffs. Below, Ill walk you through the most common PDR treatment options, the benefits and risks, and how to decide which one fits your life.
QuickStart Guide
First things first: when you get a diagnosis, you want to act fast. Delaying treatment can turn a manageable situation into permanent vision loss. Heres a snapshot of the when and why for each scenario.
| Situation | Why Treatment Matters | Typical Timeline |
|---|---|---|
| Newonset neovascularization | Prevent vitreous bleed and rapid vision loss | Within weeks of diagnosis |
| Persistent macular edema | Protect central vision where you read and drive | As soon as OCT shows fluid |
| Prior laser scar tissue | Reevaluate need for adjunct therapy | At followup (36months) |
These three scenarios cover most peoples early questions. If you recognize any of them, its time to talk to a retinal specialist.
Core Treatment Modalities
PanRetinal Photocoagulation (PRP)
What it is. PRP is a laser technique that sprays tiny burns across the peripheral retina. The burns shrink the oxygenstarved tissue thats screaming for blood vessels, which in turn lowers the growthfactor signal that fuels neovascularization.
How it works. A study in the showed that PRP reduces the chance of severe vision loss by more than 50%.
Benefits. Its a triedandtrue method that often needs only one or two sessions. Once the laser is done, the risk of bleeding drops dramatically.
Risks. Because PRP targets the peripheral retina, you may notice a dimmer night vision or a slightly narrower visual field. Some patients also develop temporary swelling in the macula.
What to Expect During PRP
- Pretreatment exam: OCT and fluorescein angiography map the leaking vessels.
- The laser session: Usually under a mild anesthetic eye drop; each spot lasts a split second, but the whole procedure can run 1530minutes.
- Postlaser care: Your doctor may prescribe antiinflammatory drops for a week and advise you to avoid bright lights for a day or two.
Expert Insight
When I chatted with Dr. Maya Hsu, a retinal laser specialist at a major academic center, she emphasized that PRP is still the backbone of PDR care because it tackles the root causeoxygen deprivation. The key is to monitor the patient closely for any macular changes after the session.
AntiVEGF Intravitreal Injections
What it is. AntiVEGF drugs (like aflibercept, bevacizumab, ranibizumab, and the newer faricimab) are tiny molecules injected directly into the eye. They neutralize the vascular endothelial growth factor (VEGF) that fuels new, leaky vessels.
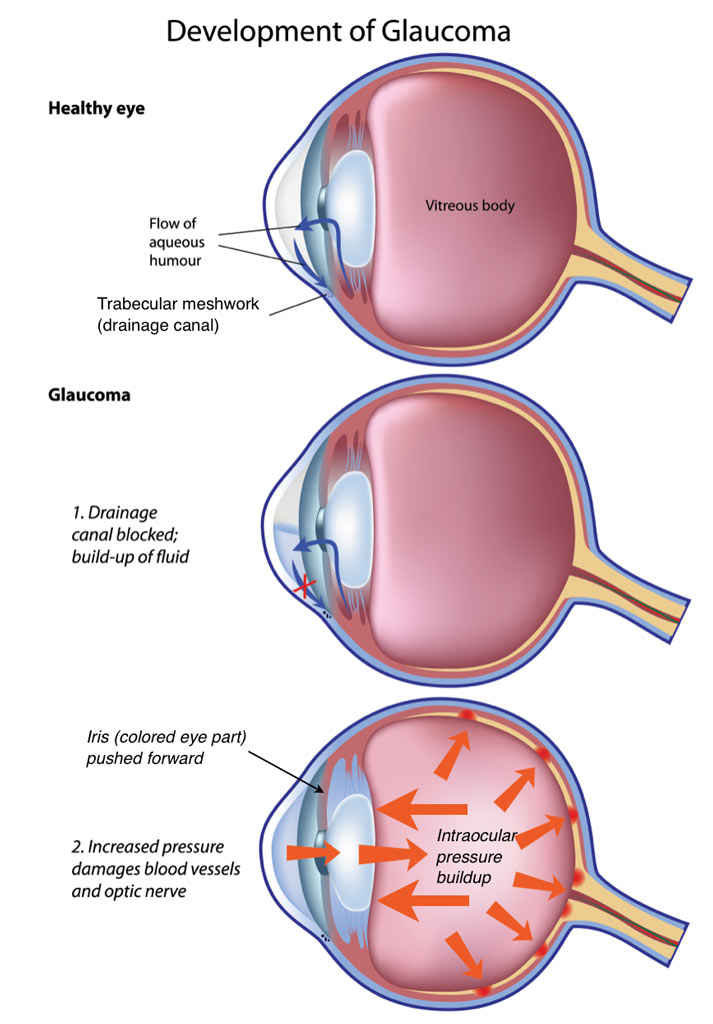
When it shines. If you have a lot of growth in the central retina (macular edema) or youre worried about losing night vision, antiVEGF may be the first choice. Many retinal specialists now also consider adjunct approaches for patients who develop glaucoma-like complications; for example, neovascular glaucoma symptoms such as painful red eye and rapid vision deterioration require urgent attention and may change the treatment plan to include interventions aimed at controlling intraocular pressure as well as the proliferative disease. For more on those warning signs, see neovascular glaucoma symptoms.
Pros. Vision often improves within 12weeks, and peripheral vision is preserved.
Cons. Injections are usually needed every month or every few months, the cost can add up, and theres a tiny risk of infection (endophthalmitis).
PRP vs. AntiVEGF: Quick Comparison
| Feature | PRP | AntiVEGF |
|---|---|---|
| Frequency | 13 sessions | 14 injections/yr |
| Immediate vision impact | Possible temporary loss | Often improves |
| Nightvision | Reduced | Preserved |
| Cost per year (US) | $1,000$2,000 | $4,000$8,000 |
| Ideal for | Peripheral lesions | Central edema + neovascularization |
According to the , antiVEGF injections have become the firstline therapy for many patients with PDR because they address both new vessels and swelling.
RealWorld Story
John, 58, was diagnosed with mild NPDR (nonproliferative diabetic retinopathy). Within two years, his eye doctor saw proliferative changes creeping in, and Johns vision dropped to 20/80. He switched from PRP to aflibercept, received five injections over six months, and his acuity climbed back to 20/30. It felt like the world got sharper again, John told me, and I could finally read my grandkids bedtime stories.
Vitrectomy (Surgical Removal of Vitreous Hemorrhage)
Why youd need it. When bleeding doesnt clear on its own or when scar tissue pulls on the retina (tractionretinal detachment), surgery may be the only way to restore sight.
What happens. A tiny, highspeed cutter removes the cloudy vitreous gel and any blood, often followed by a targeted laser burn to seal any remaining leaky vessels.
Success rate. Recent data from the suggest 8090% of eyes regain functional vision after vitrectomy for PDR.
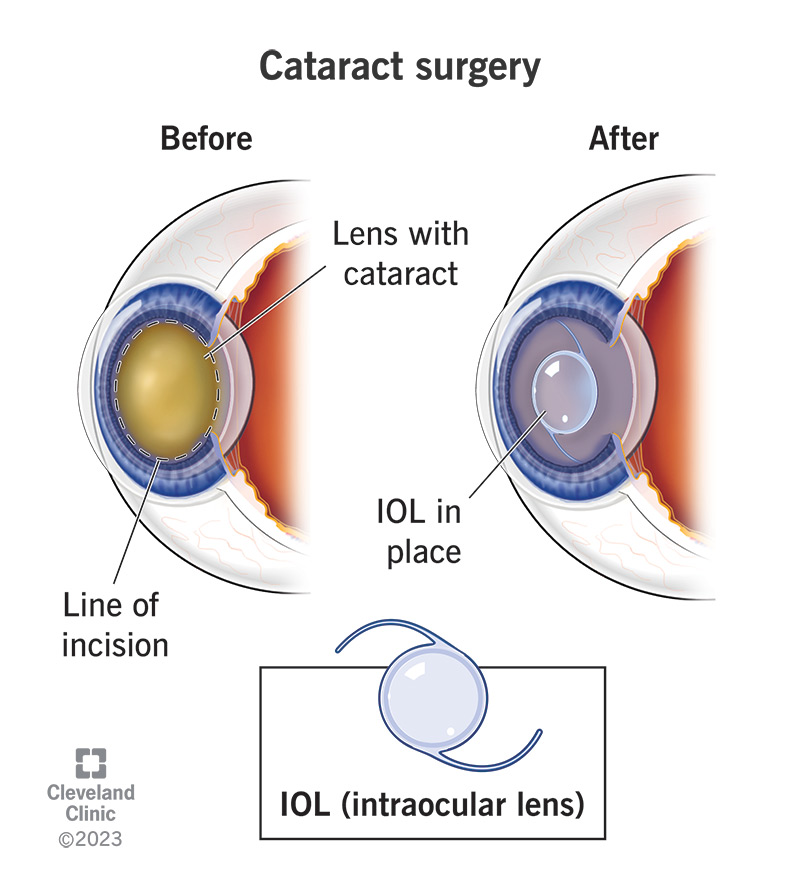
Risks. Cataract formation (especially in phakic eyes), retinal breaks, and postoperative inflammation are the main concerns.
Recovery Roadmap
- Day of surgery: Youll get antibiotic and steroid eye drops; most people go home the same day.
- Week1: Keep the eye patched for a few hours, avoid heavy lifting, and use prescribed drops.
- Month13: Gradual return to reading, driving (once cleared), and followup OCT scans to monitor healing.
Authority Boost
Dr. Luis Gonzalez, a vitreoretinal surgeon, notes, Vitrectomy is a gamechanger for eyes where the blood has turned the visual field into a fog. When combined with postop antiVEGF, the outcomes are even better.
Emerging & Adjunct Treatments
Combination Therapy (PRP+AntiVEGF)
Many doctors now start with antiVEGF to quickly shrink the vessels, then follow up with PRP for longterm stability. This twopronged approach leverages the fast visual recovery of injections and the durability of laser.
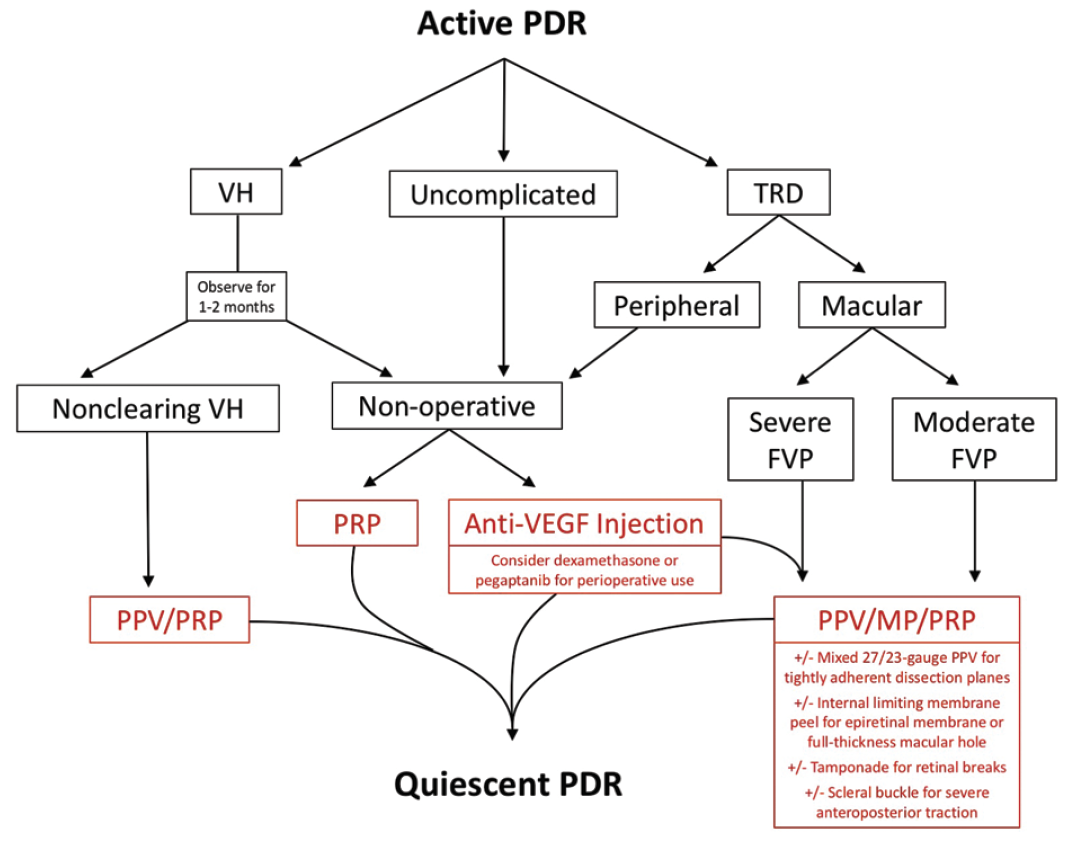
DecisionMaking Flowchart (Visual Aid)
Imagine a simple flow: New PDR Start antiVEGF Reevaluate in 46weeks If still active, add PRP. This roadmap keeps you from overlasering while still protecting against future bleeds.
New Pharmacologic Options (Faricimab, Brolucizumab)
Faricimab is a dualtarget drug that blocks VEGF and Ang2, potentially extending the interval between injections to 1216 weeks. Early phaseIII trials show promising results, though its still pending broader FDA approval for PDR.
Expert Commentary
These nextgen agents could reduce the treatment burden dramatically, says Dr. Alan Lee from the University of Michigan, who presented the data at the 2025 Retina Conference.
Lifestyle & Systemic Control
All the eyelevel treatments in the world wont help if your blood sugar stays high. Tight glycemic control (A1C<7%), blood pressure management, and lipid control cut the progression risk by up to 60%.
QuickTips Box
- Check your A1C every 3 months.
- Maintain a balanced diet rich in leafy greens and lowglycemic carbs.
- Exercise 150minutes a weekyour eyes thank you.
How to Choose the Right Option for You
Choosing a treatment isnt just about the science; its about your lifestyle, budget, and how you feel about needles. Heres a stepbystep way to decide:
- Assess disease severity: Your doctor will use OCT, fluorescein angiography, and visualfield tests.
- Consider personal lifestyle: Can you make monthly injection appointments? Are you okay with a possible nightvision dip?
- Review insurance & cost: PRP is usually covered; antiVEGF may need prior authorization.
- Discuss openly with your retinal specialist: Bring this list of questions (feel free to copy from the FAQ section above).
Printable DecisionAid Worksheet
Download a simple PDF that lets you tick boxes for each factorhelps keep the conversation focused.
Bottom Line Balancing Benefits & Risks
- PRP: Timetested, oneorfew sessions, but may dim night vision.
- AntiVEGF: Fast visual gains, preserves peripheral vision, but needs repeated visits and higher cost.
- Vitrectomy: Surgical fix for stubborn bleeding or traction, excellent outcomes when needed.
- Combination therapy: Often the sweet spot for complex cases.
Ultimately, the best path is the one that protects your sight while fitting comfortably into your life. Early action, regular eye exams, and open dialogue with your doctor are the real superpowers.
Conclusion
Proliferative diabetic retinopathy isnt a life sentencethanks to laser, antiVEGF drugs, and modern surgery, you have multiple evidencebacked ways to protect your sight. The key is knowing what each option does, its risks, and how it fits your daily routine. Talk openly with your retinal specialist, weigh the pros and cons, and keep your overall health in check. Got more questions? Drop a comment below or reach out to your eye doctor todayyour vision deserves that conversation.
FAQs
What is the first‑line treatment for proliferative diabetic retinopathy?
Pan‑retinal photocoagulation (PRP) remains the traditional first‑line therapy because it quickly reduces the oxygen‑starved stimulus that drives abnormal vessel growth.
How do anti‑VEGF injections compare to laser therapy?
Anti‑VEGF injections often improve vision within weeks and preserve night vision, but they require repeated office visits. Laser (PRP) typically needs only one‑to‑three sessions but can dim peripheral and night vision.
When is vitrectomy recommended for PDR?
Vitrectomy is advised when there is non‑clearing vitreous hemorrhage or traction‑induced retinal detachment that threatens central vision and cannot be managed with laser or injections alone.
Can lifestyle changes slow the progression of PDR?
Yes. Tight blood‑sugar control (A1C < 7 %), blood‑pressure management, and a healthy diet can reduce the risk of progression by up to 60 %.
How often will I need follow‑up appointments after treatment?
After PRP, a follow‑up at 1‑3 months is typical to check for residual disease. Anti‑VEGF regimens often require monthly or bimonthly visits initially, then spaced out based on stability. Vitrectomy patients usually see their surgeon at 1 week, 1 month, and then every 3‑6 months.