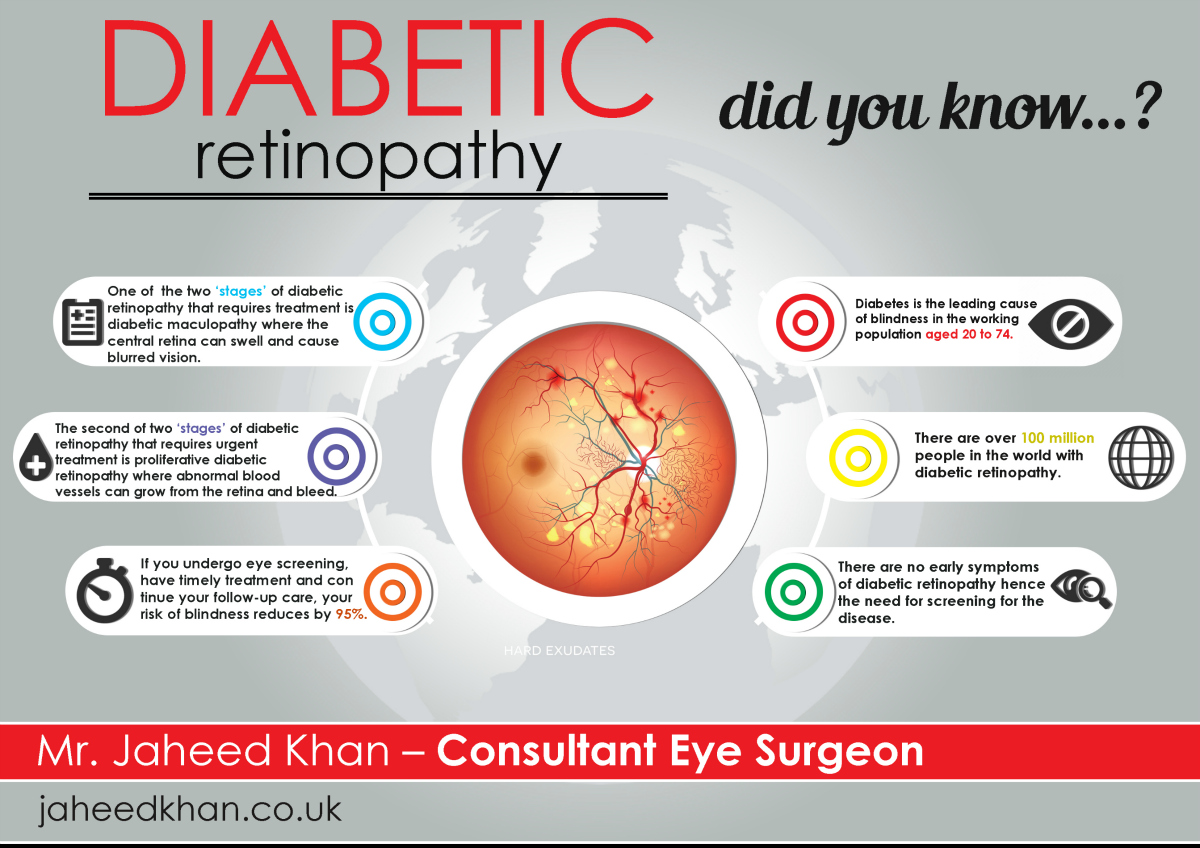
Bottom line: In the very first stage of diabetic eye disease the tiny blood vessels in your retina start to leak or balloon out, but you often feel nothing at all. Catching it early through a quick dilated eye exam lets doctors treat it before vision ever blurs.
Why it matters: Even though most people think no symptoms = no problem, the wall-weakening that begins weeks or months before you notice floaters can be slowed or even reversed with laser or anti-VEGF therapy, tight blood-sugar control, and regular checkups. Lets walk through what that looks like, step by step.
How It Starts
What actually happens to retinal blood vessels?
Think of the retina as a delicate fabric woven with thousands of microscopic blood tubes. When blood-sugar stays high, those tubes get stressed: they swell, develop tiny outpouchings called microaneurysms, and sometimes leak fluid. Over time the fabric gets a little wet spot, which is the first sign of early diabetic retinopathy.
According to a , the process begins silentlyoften months before you're even aware of any change.
Why most people get it wrong
We love shortcuts, so the myth that you'll only notice problems when vision gets fuzzy spreads fast. In reality, the early stage is usually asymptomatic, meaning you can have damage without any warning sign. That's why routine eye exams are the real hero here.
First Signs
What is the first sign of diabetic retinopathy?
The first visual clue is usually a handful of tiny, pale spots on the retina that you can't see without specialized imaging. For you, the first tangible hint might be occasional floaterstiny specks that drift across your field of view, especially when you look at a bright background.
Can you feel any symptoms?
Most people feel nothing. If you start noticing blurred vision, difficulty distinguishing colors, or a sudden increase in floaters, those are red flags that the retinopathy may be moving beyond the early stage.
Real-world anecdote
Take Maya, a 45-year-old accountant who thought no pain, no problem applied to her eyes. A routine check-up revealed several microaneurysms. She was surprisedshe hadn't noticed any vision change. After a few laser sessions and tighter glucose monitoring, her retinal health stabilized, and she never needed more aggressive treatment.
Diagnosis Process
What tests are used?
The gold standard is a dilated eye exam, where drops widen your pupils so the doctor can see the back of your eye. In addition, doctors often use:
- Optical Coherence Tomography (OCT) a cross-sectional scan that shows swelling.
- Fluorescein Angiography a dye-based test that highlights leaking vessels.
How accurate are these tests?
Recent studies show OCT can detect early retinal thickening with a sensitivity of about 92% and specificity around 88% (). Fluorescein angiography, while more invasive, catches even the smallest leaks.
| Test | What It Shows | Sensitivity | Typical Use |
|---|---|---|---|
| Dilated Exam | Overall retinal health, visible microaneurysms | ~85% | First-line screening |
| OCT | Retinal thickness, fluid accumulation | 92% | Detecting early swelling |
| Fluorescein Angiography | Leakage patterns, vessel blockage | 95% | Confirming extent of damage |
Where does early fit?
In the eye-doctor's staging system, early corresponds to mild nonproliferative diabetic retinopathy (NPDR). At this point you'll see a few dot-like hemorrhages or microaneurysms, but no new vessels have formed yet.
Disease Staging
From mild to proliferative quick overview
The retina's disease journey is usually broken into four stages:
- Mild NPDR a few microaneurysms.
- Moderate NPDR more hemorrhages, some cotton-wool spots.
- Severe NPDR many lesions, risk of new vessel growth.
- Proliferative Diabetic Retinopathy (PDR) new, fragile vessels form, risking bleeding.
Why early matters
Intervening at the mild stage can keep you far away from proliferative diabetic retinopathy, which is the form that often leads to vision-threatening bleeding or retinal detachment.
Treatment Options
Can diabetic retinopathy be reversed?
Reversal is a loaded word. The damage that's already scarred can't be undone, but the disease's progression can be halted, and in many cases early signs can improve. Clinical trials show that focal laser photocoagulation and anti-VEGF injections can shrink leaking vessels and reduce fluid, effectively reversing the active disease process.
First-line therapies
Before any laser or injection, the most powerful tool is lifestyle:
- Blood-sugar control keeping A1C under 7% reduces risk by up to 40% ().
- Blood-pressure management under 130/80 mmHg slows retinal damage.
- Lipid control statins can lower the chance of new vessel growth.
When is laser needed?
If OCT or angiography shows persistent leakage despite good glucose control, doctors may recommend focal/grid laser. The procedure takes about 10 minutes, feels like a brief flicker, and you'll need to avoid bright light for a day or two.
Step-by-step of a typical laser session
- Eye drops dilate the pupil.
- Doctor positions a special contact lens on the eye.
- Laser pulses target leaking spotseach pulse feels like a tiny snap.
- Post-procedure: Use sunglasses and avoid straining the eyes for 2448 hours.
Anti-VEGF injections
For more aggressive early signs, anti-VEGF (vascular endothelial growth factor) drugs are injected directly into the eye. They block the chemical that tells new vessels to grow. Most patients need a series of three monthly injections, then a maintenance schedule.
Lifestyle Management
How diet & exercise impact retinal health
Think of your eyes as a garden; they need steady water (glucose) but not a flood. A Mediterranean-style dietrich in leafy greens, fish, nuts, and olive oilhas been linked to slower retinal degeneration. Regular brisk walking (30 minutes a day) improves circulation, delivering oxygen to those fragile vessels.
Which meds raise risk?
Some steroids and certain antihypertensives can aggravate leakage. Always ask your primary care doctor if a medication could affect your eye health.
Monitoring schedule
When you're in the early stage, an eye exam every 12 months is typical. If you have type 1 diabetes or a longer disease duration, aim for every 6 months. Your doctor will adjust the frequency based on how your retina looks.
When to Seek Help
Red-flag symptoms that demand immediate care
If you notice any of these, call your eye doctor right away:
- Sudden appearance of many floaters.
- Flashes of light, especially in peripheral vision.
- Rapidly worsening blurry vision.
- Dark spots that seem to grow.
How to prepare for your dilated exam
Bring a list of all medications, a recent blood-sugar log, and wear sunglasses for the post-exam light sensitivity. Arriving a few minutes early lets you relax and ask any lingering questions.
Trusted Resources & Further Reading
Key sites to bookmark
When you want a deeper dive, these sources are reliable:
Suggested professional contacts
Consider building a small eye-health squad: an optometrist for routine screenings, a retinal specialist for any advanced findings, and a certified diabetes educator to keep your numbers in check.
Conclusion
Early diabetic retinopathy is sneakyoften symptom-freebut spotting those tiny retinal changes early can mean the difference between a simple laser session and permanent vision loss. By getting regular dilated exams, keeping blood-sugar and blood-pressure on point, and acting fast on any new floaters or flashes, you can halt or even improve the disease's trajectory. Schedule your next eye checkup today, and feel free to share your own story or questions in the comments belowyou're not alone on this journey.
For additional context on related eye conditions that can affect vision, consider reading about dry eye disease and how surface irritation can complicate management of retinal conditions.
FAQs
What is early diabetic retinopathy?
Early diabetic retinopathy is the first stage of diabetic eye disease where tiny blood vessels in the retina begin to leak or form micro‑aneurysms, usually without any noticeable symptoms.
How is early diabetic retinopathy diagnosed?
It is detected through a dilated eye exam, often supplemented with Optical Coherence Tomography (OCT) and fluorescein angiography, which reveal micro‑aneurysms, retinal thickening, and tiny leaks.
Can early diabetic retinopathy be treated?
While existing scar tissue cannot be undone, progression can be halted or improved with tight blood‑sugar control, laser photocoagulation, and anti‑VEGF injections when leakage persists.
How often should I get eye exams if I have early diabetic retinopathy?
Most specialists recommend an eye exam every 12 months, but individuals with type 1 diabetes or longer disease duration may need exams every six months.
What lifestyle changes help slow early diabetic retinopathy?
Maintaining A1C below 7%, controlling blood pressure, following a Mediterranean‑style diet, regular exercise, and avoiding smoking are key to protecting retinal health.