Quick answer: The FIGO system classifies ovarian, fallopiantube and peritoneal cancers into stagesIIV (with substagesAC). The most recent 2025 draft adds microscopic peritoneal implants and precise lymphnode rules, making the stage a clearer guide for surgery, chemotherapy and survival outlook. Knowing your ovarian cancer staging figo is the first step toward the right treatment plan.
Staging Overview
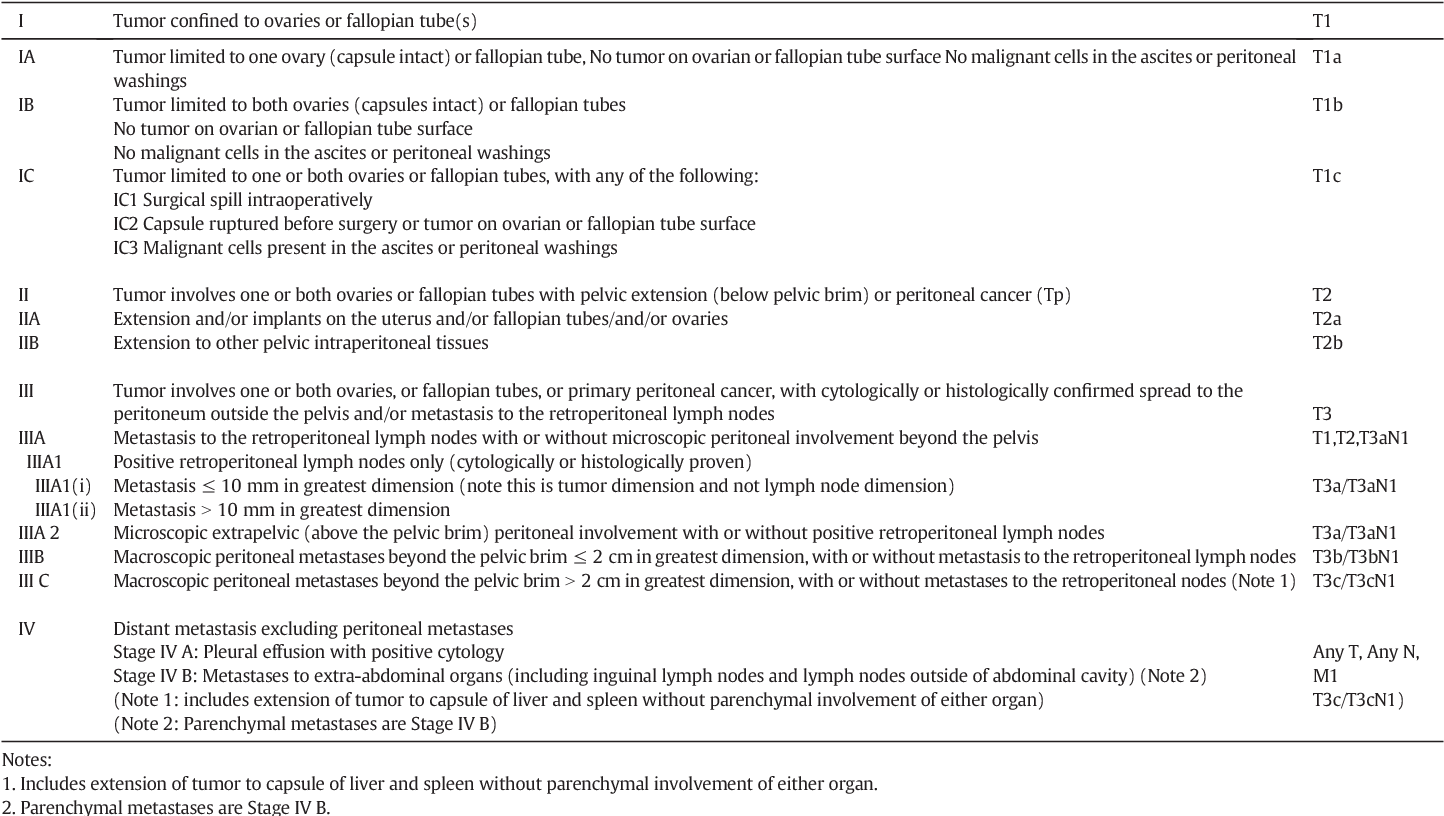
Lets start with the basicswhat does each FIGO stage actually mean? Below is a concise rundown that you can refer to whenever you hear stageII or stageIIIC in a clinic.
| Stage | Definition (2025 draft) | Typical Treatment |
|---|---|---|
| IA | Tumor limited to one ovary; capsule intact; no tumor on surface. | Unilateral salpingooophorectomy; observation or limited chemo. |
| IB | Both ovaries involved, no surface spread. | Total hysterectomy + bilateral salpingooophorectomy. |
| IC (AC) | IC1 surgical spill; IC2 capsule rupture before surgery; IC3 surface tumor or positive washings. | Comprehensive surgery + adjuvant chemo. |
| IIAB | Extension to uterus or fallopian tubes (A) or other pelvic organs (B). | Optimal cytoreduction; chemo. |
| IIBC | IIA/B with implants 2cm (C) or >2cm (C). Includes diaphragm peritoneum. | Aggressive debulking; chemo. |
| IIIAC | Microscopic peritoneal spread beyond pelvis. | Extensive surgery; platinumbased chemo. |
| IIIBC | Macroscopic peritoneal implants 2cm (B) or >2cm (C) on the abdomen. | Complete cytoreduction if possible; chemo. |
| IIICN | Positive retroperitoneal or inguinal lymph nodes (any size). | Node dissection + chemo; sometimes HIPEC. |
| IV | Distant metastasis (liver parenchyma, lungs, etc.) | Systemic therapy; palliative surgery if needed. |
Notice how the 2025 draft sharpens the language around lymph nodes (the N suffix) and microscopic implants. That extra precision helps doctors pick the most effective regimen for you.
2025 Update
So why all the buzz about a new FIGO staging? The last major revision was back in 2018; the 2025 draft introduces three gamechanging tweaks.
- Nodepositivity rule: Any confirmed metastatic lymph nodeno matter how tinyelevates the stage to IIICN. It sounds technical, but its simply acknowledging that even a single rogue node can affect prognosis.
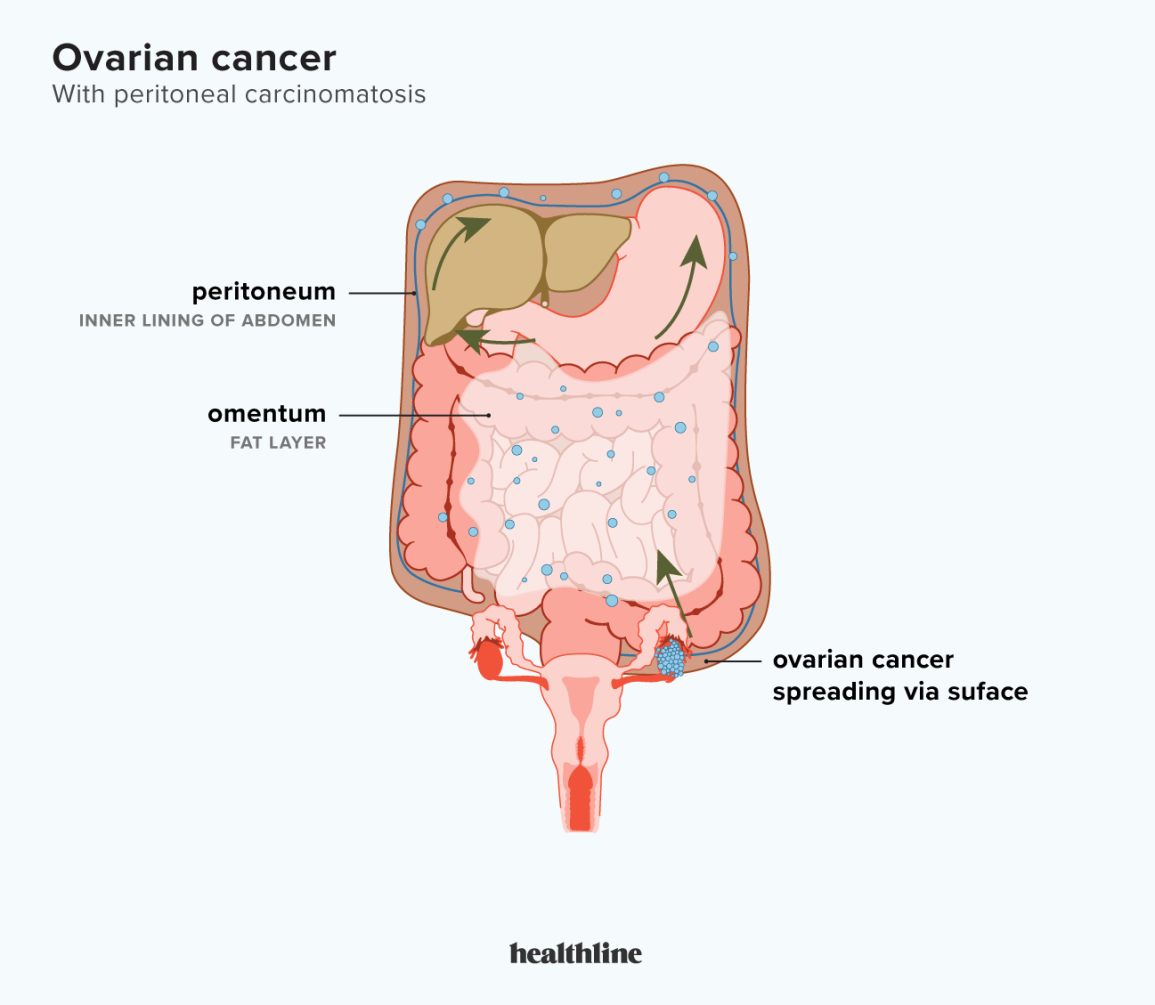
- Unified primary site: Ovarian, fallopiantube, and peritoneal cancers now share the same staging chart. That means the same stage conveys the same meaning, no matter where the tumor started.
- Radiologic tieins: The draft recommends specific CT, MRI and PETCT findings for each stage, making the imaging report a direct bridge to the surgical plan.
Dr. Elena Ramirez, a gynecologic oncologist I chatted with last month, summed it up nicely: The 2025 revision is less about reinventing the wheel and more about adding the missing spokesespecially those little nodes that we often missed before. Her experience treating over 300 patients gave her a firsthand view of how these details shift treatment decisions.
Want the official paper? You can grab the directly from FIGOs website. Its a quick read (about 12 pages) and worth bookmarking for future appointments.
Treatment Decisions
Knowing the stage isnt just academicit directly shapes the treatment roadmap. Below is a friendly cheatsheet that maps each major stage to the most common surgical and medical options.
Stage I (AC)
When the disease is still confined to the ovaries, many doctors aim for fertilitypreserving surgery if youre of childbearing age. A unilateral salpingooophorectomy (removing one ovary and its tube) can be enough for IA. For IC, most clinicians add a short course of carboplatin and paclitaxel to mop up any microscopic spread.
Stage II (AC)
Now the tumor has ventured into the pelvis. The goal becomes optimal cytoreductionremoving as much visible tumor as possible, often leaving no residual disease larger than 1cm. After surgery, the standard is six cycles of platinumbased chemotherapy. If youre lucky and the surgeon achieves no visible tumor, some studies suggest you might skip a few chemo cycles, but thats still being debated.
Stage III (AC, N)
This is where the battle intensifies. The abdomen is often peppered with implants, and the lymph nodes may be involved. , the preferred approach is maximal debulking followed by at least six cycles of carboplatin+paclitaxel. In many centers, a dosedense schedule (administering chemo every two weeks) shows better progressionfree survival.
For patients with a confirmed IIICN, many surgeons also perform a systematic lymphadenectomyremoving suspicious nodes to improve staging accuracy. Some highvolume hospitals are experimenting with hyperthermic intraperitoneal chemotherapy (HIPEC) right after surgery; early data look promising but are still under investigation.
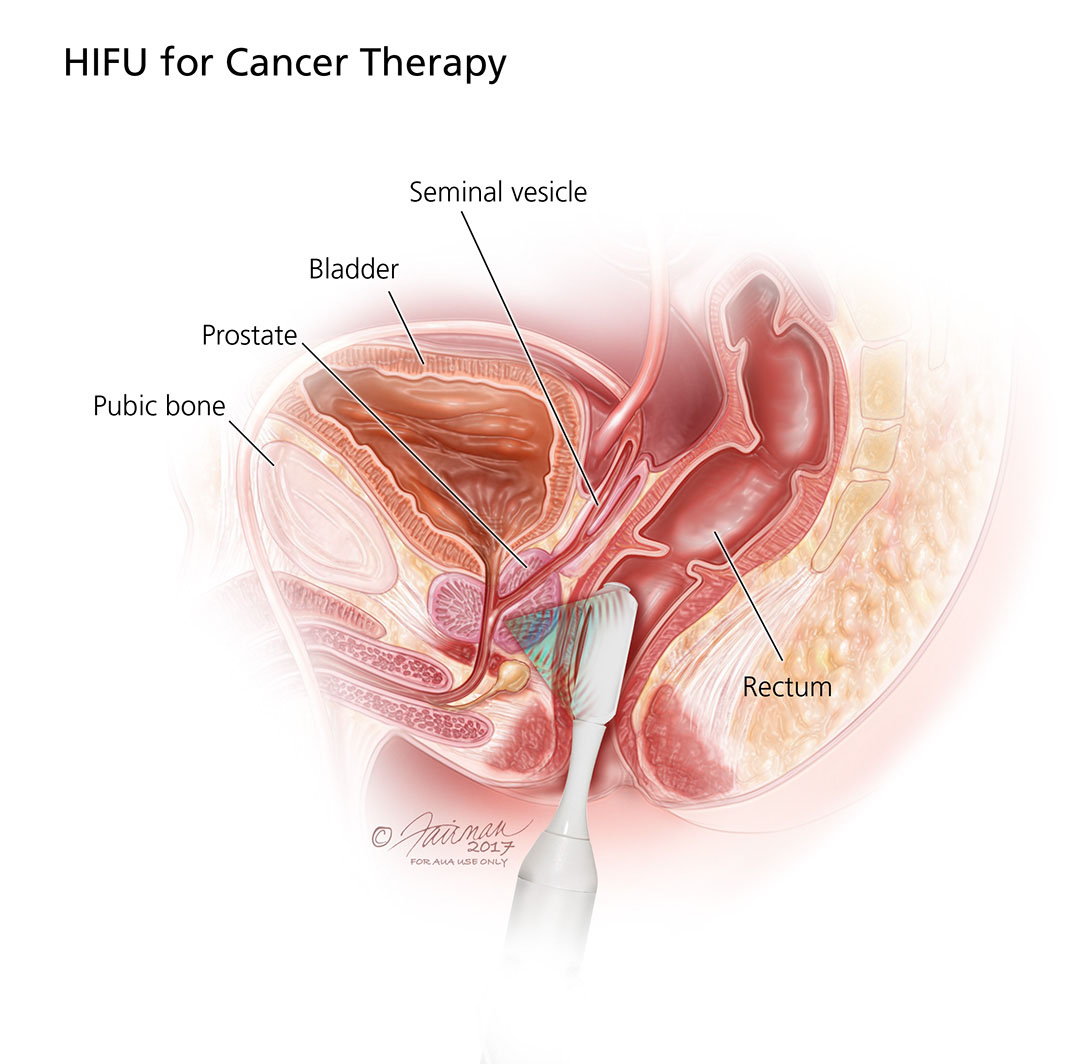
Patients and caregivers often also research related cancer topics while planning care for example, those navigating prostate cancer decisions sometimes compare survival metrics across cancers; resources on prostate cancer outlook can be useful context when discussing longterm surveillance and survivorship planning.
Stage IV
Distant metastasis means the cancer has spread beyond the abdomencommonly to the liver, lungs, or brain. Treatment shifts to systemic therapy: platinumbased chemo combined with targeted agents like PARP inhibitors (olaparib, niraparib) or bevacizumab. Clinical trials are abundant, and enrolling can give access to cuttingedge drugs.
Prognosis Snapshot
Survival chances vary widely. a fiveyear survival of about 90% for stageI, dropping to roughly 4050% for stageIII, and under 20% for stageIV. Those numbers are averages; your personal outlook depends on age, overall health, tumor biology, and how aggressively the cancer responds to treatment.
Practical Tools
Now that youre armed with the basics, here are a few handy resources you can keep at your fingertips.
- Downloadable cheatsheet: A onepage PDF summarizing each FIGO stage, typical imaging signs, and the most common surgical approach. (Just click Download on the FIGO PDF page.)
- Interactive staging calculator: Several reputable oncology sites let you input tumor size, surface involvement, and node status to instantly see your FIGO stage. Its a useful conversation starter with your doctor.
- Radiology checklist: When reviewing your CT or MRI report, ask the radiologist if they see implant 2cm or lymphnode positivitythose phrases line up directly with the staging chart.
- Reference hub: Keep a list of credible sources (FIGO, NCCN, ACS, NCBI pathology outlines) bookmarked. When you hear a new term, youll have a trusted place to verify it.
Final Thoughts
Understanding ovarian cancer staging figo isnt just about memorizing letters and numbers; its about gaining a roadmap for your journey. The stage tells you how far the disease has traveled, which treatments are most likely to work, and what you can expect in the months ahead. It also gives you a language to ask focused questions at your next appointmentquestions like Did my scan show any lymphnode involvement that would make this a IIICN? or What does the 2025 update mean for my treatment plan?
If youre standing at the crossroads of a diagnosis, take a moment to download that , jot down the stage youre given, and bring it to your next consultation. Having that sheet in hand shows youre proactive and ready to partner with your care team.
Remember, youre not alone in this. Whether youre a patient, a caregiver, or just a curious mind, the more you understand the staging system, the better you can navigate treatment options, weigh risks, and celebrate each small victory along the way. If anything in this guide sparked a question or you want to share your own experience, feel free to reach outknowledge grows stronger when we share it.
FAQs
What does FIGO stand for in ovarian cancer staging?
FIGO stands for the International Federation of Gynecology and Obstetrics, which provides the staging system used worldwide to classify ovarian cancer based on tumor spread.
What are the main stages of ovarian cancer in the FIGO system?
Ovarian cancer is classified into stages I through IV in the FIGO system, with substages indicating specifics on tumor extent, lymph node involvement, and metastasis to distant organs.
How does lymph node positivity affect FIGO ovarian cancer staging?
Any confirmed metastatic lymph node, regardless of size, upgrades the stage to IIICN in the 2025 FIGO update, highlighting its importance in prognosis and treatment planning.
What typical treatments correspond to different FIGO stages of ovarian cancer?
Treatments vary by stage: early stages often involve surgery with possible limited chemotherapy; advanced stages require aggressive cytoreductive surgery plus platinum-based chemotherapy; stage IV focuses on systemic therapy and targeted drugs.
Why is the 2025 FIGO staging update significant?
The 2025 update refines lymph node criteria, unifies staging for ovarian, fallopian tube, and peritoneal cancers, and integrates imaging findings for better surgical and therapeutic decisions.