If you or someone you love lives with osteoporosis, a simple stumble can turn into a lifechanging hip fracture. The truth is, the sooner you recognize the risk, the better you can protect your independence and health. Below well break down why these fractures are so serious, how to spot them early, what treatment looks like, and what you can do right now to stay strong.
Understanding the Fracture
What is an osteoporosis hip fracture?
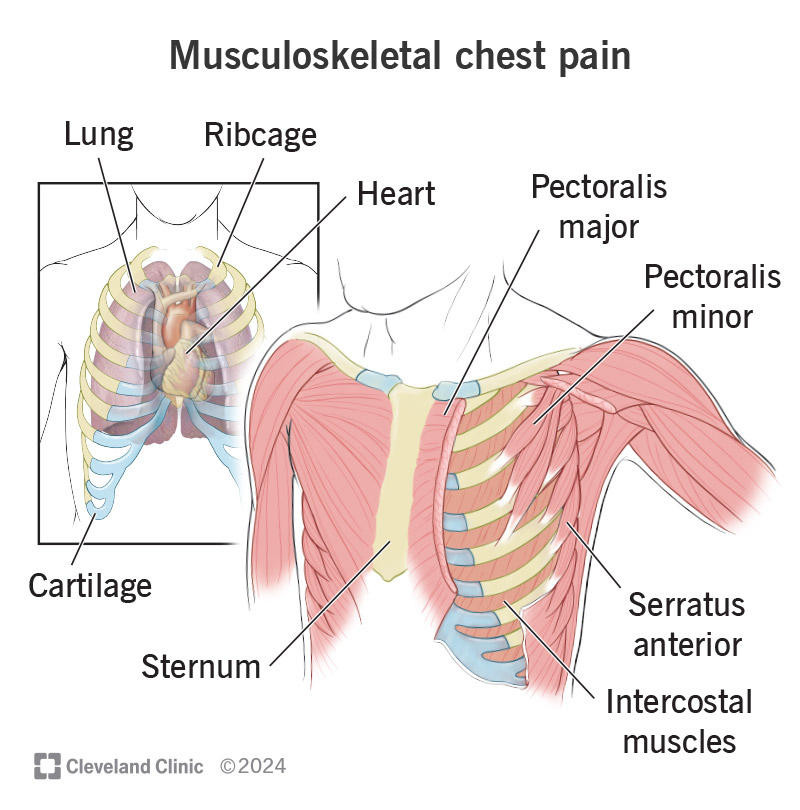
In plain language, an osteoporosis hip fracture is a break in the upper part of the thigh bone (the femur) that occurs because the bone has become porous and weak. Even a minor slip on a bathroom rug can generate enough force to crack the femur when bone density has dropped below the normal range (a Tscore of2.5 or lower). According to , the hip is one of the most vulnerable sites because it bears the bodys weight and the surrounding muscles exert powerful forces during a fall.
Pathophysiology (Nursing Perspective)
From a nursing standpoint, the fracture is the final step in a cascade that starts with bone remodeling imbalance. Osteoclasts (the cells that break down bone) become overactive while osteoblasts (the builders) fall behind, leaving the femur thin and brittle. Add agerelated changes in balance, vision, and reaction time, and the odds of a fall skyrocket. A recent nursing review highlighted that reduced calcium absorption, hormonal shifts, and chronic inflammation all play a role in the .
Types of Hip Fractures
Not all hip fractures are created equal. The three most common patterns are:
| Fracture Type | Location | Typical Mechanism | Preferred Surgery |
|---|---|---|---|
| Femoral Neck (Subcapital) | Just below the ball of the hip joint | Sideways fall, direct impact | Hemiarthroplasty or total hip replacement |
| Intertrochanteric | Between the greater and lesser trochanters | Fall onto the side, twisting | Internal fixation (screw/plate) |
| Subtrochanteric | Below the lesser trochanter | Highenergy trauma or severe osteoporosis | Long intramedullary nail |
Understanding which type youre dealing with guides the treatment plan and predicts recovery speed.
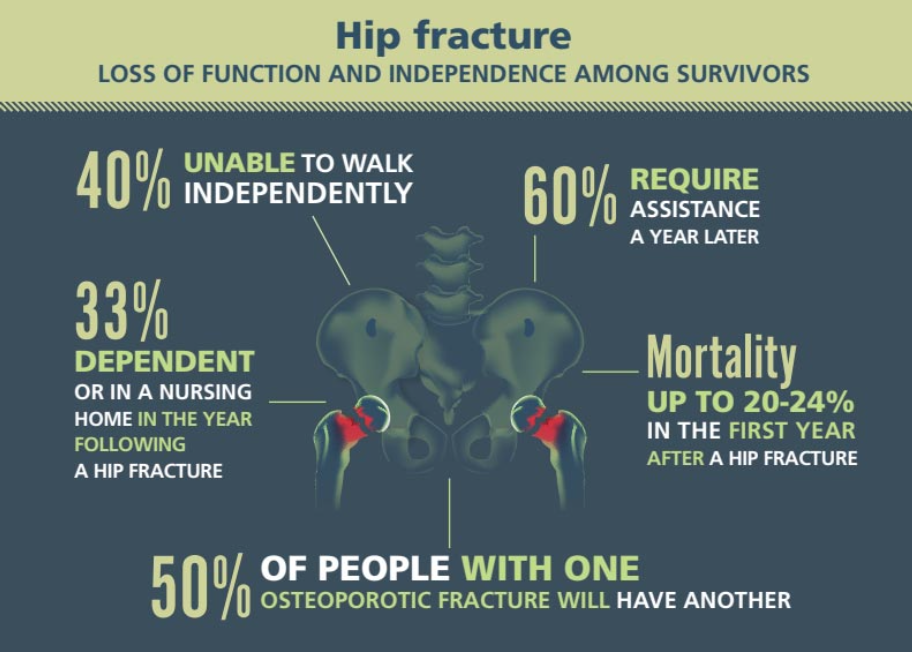
Why is a hip fracture so dangerous?
Its not just the broken bone that worries doctorsits what the break sets off. Immediately after the fracture, patients often become immobilized, which can trigger a cascade of complications: pneumonia from shallow breathing, blood clots in the legs (deepvein thrombosis), pressure sores, and even a sudden drop in blood pressure. The reports that about one in three patients with an osteoporotic hip fracture will die within a year, largely because of these secondary problems.
Spotting Hidden Symptoms
Classic vs. silent signs
Many people think a broken hip always feels like a sharp, obvious pain, but thats not always the case. Classic symptoms include:
- Sudden, severe pain in the groin or thigh
- Inability to put weight on the affected leg
- Visible bruising or a limp
However, an undiagnosed hip fracture can masquerade as a simple strain. Some older adults report a vague stiffness that doesnt improve after a few days of rest, or they may keep shuffling around with a mild ache because theyre afraid of calling for help. A study in found that up to 15% of hip fractures in seniors are initially missed, leading to delayed surgery and worse outcomes.
When to call emergency services
If you notice any of the following, treat it like a medical emergency:
- Severe pain that worsens with movement
- Inability to stand or walk even with assistance
- Extreme swelling or visible deformity around the hip
Time mattersa surgery performed within 2448hours dramatically reduces mortality and speeds up rehab.
Realworld anecdote
Take Mary, an 78yearold who slipped in her kitchen. She thought shed just bruised her hip and kept walking. Two days later, she could no longer climb the stairs without wincing. A quick Xray at the emergency department revealed an intertrochanteric fracture that had been festering. Because the diagnosis was delayed, Mary needed a longer hospital stay and faced a tougher rehab journey. Her story reminds us that just a little pain can hide a serious injury.
Treatment and Recovery
Immediate medical management
The first steps after a suspected fracture are pain control (often with IV opioids or nerve blocks) and imaging. While Xrays catch most breaks, an MRI can reveal cracks that are invisible on plain film, especially in the early occult stage.
Surgical options
Choosing the right surgery depends on the fracture type, the patients age, and overall health. The main options are:
- Internal fixation: Screws or plates hold the bone together; best for younger, active patients with clean breaks.
- Hemiarthroplasty: Replaces the ball of the hip; common for older adults with femoralneck fractures.
- Total hip replacement: Replaces both ball and socket; reserved for patients who were mobile before the injury.
Pros & Cons of Surgery vs. NonSurgical Care
| Approach | Advantages | Disadvantages |
|---|---|---|
| Surgery (Fixation/Replacement) | Early mobilization, lower longterm pain, better functional outcome | Operative risks (infection, anesthesia), higher initial cost |
| Conservative (NonSurgical) | Avoids surgical risks, suitable for very frail patients | Prolonged bed rest, higher chance of complications, often poorer mobility |
Postoperative rehabilitation
Physical therapy starts within the first 24hours for most patients. Goals include:
- Gentle rangeofmotion exercises for the hip and knee
- Weightbearing as tolerated (often with a walker)
- Strengthening the glutes and core to improve balance
Research shows that patients who begin rehab early are twice as likely to walk independently after six weeks.
Medication for bone health after a fracture
Repairing the bone is only half the battle; you also need to treat the underlying osteoporosis. Options include:
- Bisphosphonates (e.g., alendronate)
- Denosumab, a monoclonal antibody given every six months
- Anabolic agents such as teriparatide for severe bone loss
A 2024 found that initiating bisphosphonate therapy within six weeks of surgery cut the risk of a second fracture by 40%.
Nutrition and lifestyle for healing
What you put on your plate matters. Aim for at least 1,200mg of calcium and 8001,000IU of vitaminD daily, plus plenty of protein (1g per kilogram of body weight). Staying hydrated and avoiding smoking also speed recovery.
Risks and Complications
Common complications
Even with optimal care, a hip fracture can trigger a handful of serious issues:
- Infection: Surgical site infections can delay healing.
- Nonunion: The bone fails to fuse, often needing a second operation.
- Avascular necrosis: Loss of blood supply to the femoral head, especially after femoralneck fractures.
- Deepvein thrombosis (DVT): Blood clots form in the leg veins; prophylactic anticoagulants are standard.
- Pneumonia: Reduced breathing depth during bed rest.
Worst type of hip fracture
The subtrochanteric and comminuted (multiplefragment) fractures carry the highest morbidity. Their location makes fixation technically challenging, and theyre often associated with massive blood loss and longer surgical times. Consequently, patients with these fracture patterns experience higher rates of reoperation and mortality.
What causes death after a hip fracture?
Its rarely the broken bone itself thats fatal. Rather, the cascade of complicationsespecially pneumonia, heart failure, and sepsistakes a toll on an already frail system. A systematic review in noted that more than half of postfracture deaths are linked to preventable complications, underscoring the importance of early mobilization and comprehensive geriatric care.
Strategies to lower complication risk
Heres a quick checklist you can share with caregivers:
- Start gentle breathing exercises within the first 12hours.
- Apply compression stockings and administer anticoagulants as ordered.
- Schedule physicaltherapy sessions at least twice daily.
- Monitor skin for pressure points and reposition every two hours.
- Review all medications for those that increase fall risk (e.g., sedatives).
Prevention Strategies
Bone health basics
Regular bone density testing (DXA scans) is the gold standard. If your Tscore falls below2.5, talk to your physician about initiating therapy right away. Early detection gives you the chance to strengthen bone before a fracture occurs. For guidance on improving bone strength and rehabilitation after fractures, consider resources on osteoporosis physical therapy that outline practical exercise plans and recovery milestones.
Exercise that works
Weightbearing activities (walking, stair climbing) stimulate bone formation. Balancefocused classes such as TaiChi or gentle yoga reduce fall risk by up to 30%. Even a 15minute daily routine of chair stands, heel raises, and sideleg lifts can make a big difference.
Home safety audit
Take a quick walk through your home and ask these questions:
- Are there sturdy grab bars in the bathroom?
- Is the lighting adequate on stairways?
- Are rugs nonslip or removed?
- Are cords from phones or chargers tucked away?
Minor tweaks can dramatically lower the chance of a slipandfall.
Medication review
Some prescriptionslike certain blood pressure meds, sleep aids, or antihistaminescan cause dizziness. Have a pharmacist or your doctor review your list annually, especially after any new drug is added.
Ask Your Doctor checklist
| Question | Why It Matters |
|---|---|
| Should I start a bonestrengthening medication? | Targets the root cause, not just the symptom. |
| What fallprevention exercises are best for me? | Personalized plans improve adherence. |
| Do any of my meds increase my fall risk? | Minimizing sedatives can boost safety. |
Conclusion
Facing an osteoporosis hip fracture can feel overwhelming, but knowledge is power. By recognizing the warning signs early, understanding treatment pathways, and committing to bonestrengthening habits, you can dramatically improve outcomes and keep moving forward. If you have questions, share your thoughts in the comments or talk to a healthcare professional todayyou dont have to navigate this alone.
FAQs
What are the early signs of an osteoporosis hip fracture?
Sudden groin or thigh pain, difficulty bearing weight, a limp, or persistent stiffness that doesn’t improve after a short rest can indicate a fracture.
How is an osteoporosis hip fracture diagnosed?
Initial X‑rays are standard; if they are inconclusive, an MRI or CT scan can reveal occult cracks. A physician will also assess medical history and fall risk.
What treatment options are available for hip fractures caused by osteoporosis?
Most patients need surgery—either internal fixation, hemi‑arthroplasty, or total hip replacement—followed by pain control, early mobilization, and bone‑strengthening medication.
How long does recovery typically take after hip fracture surgery?
Patients usually begin gentle physical therapy within 24 hours. Full independence may take 3‑6 months, depending on age, health, and adherence to rehab.
What can I do to prevent future osteoporosis hip fractures?
Maintain adequate calcium and vitamin D, engage in weight‑bearing and balance exercises, review medications that affect balance, and make home safety modifications such as installing grab bars and removing loose rugs.